Which is more important for your health – exercise or diet? If you listen to the likes of Michelle Obama 1, then it would appear that exercise Trumps diet (pun intended and immediately regretted). This opinion appears to be shared by all those who have an interest in making money out of manufacturing/selling processed and junk food, those who want us to keep popping the pharmaceuticals and paying for mere management of our chronic illnesses rather than cure, and also by those who own gyms or sell home gym equipment and the plague of protein powders. But what do WFPB doctors and scientific research tell us?
WFPB doctors – exercise vs diet
I know that I go on and on about diet, devoting only a relatively small amount of blog space for exercise-related issues. Interestingly, it appears that I share this tendency with Dr Thomas Campbell: “…when I discuss lifestyle with my patients I spend almost all my time talking about food. My new book, The Campbell Plan 2 , contains just about a page on exercise. Am I delinquent? Perhaps I am. We know how crucial exercise is, but what I see more often than not is an overemphasis on exercise. I tend to see people focus their energies on getting to the gym as their primary strategy for weight control while leaving their diet largely the same. Perhaps they are trying to eat less, or just not snack on the junk in the house as often. Overall, this is a poor strategy.” 3 .
On the other hand, you’ll see Dr Michael Greger bounding along on his treadmill when doing his regular YouTube Q&A sessions, and he includes exercise as an integral part of his Daily Dozen 4 : “I advise one daily “serving” of exercise, which can be split up over the day. I recommend ninety minutes of moderate-intensity activity each day, such as brisk (four miles per hour) walking or, forty minutes of vigorous activity (such as jogging or active sports) each day. I explain my reasoning for that in my video, How Much Should You Exercise?” 5
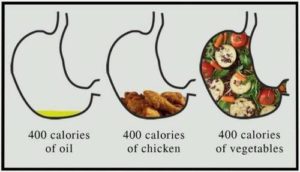
Dr Joel Fuhrman considers 6 that exercise has a lot more value than simply helping us to lose weight by more quickly burning calories: “The calories burned during exercise, unless you’re a professional athlete, make up a very small portion of our total calories burned for the day; what we eat has a much greater influence on our body weight. So why should we bother to exercise? The answer is that burning calories is just one of the many benefits of exercise.
“For example, in the chapter titled “Nutritional Excellence, Not Drugs” in my book, The End of Heart Disease 7 , I discuss how exercise is an important component in attaining excellent health: ‘When you change to a Nutritarian diet-style, cut the salt out of your diet, exercise regularly, and lose weight, you remove inflammation, reduce atherosclerosis, and eliminate the inflammation of the endothelium. In other words, the causes of high blood pressure are eliminated, and the blood vessels begin to heal themselves.’ ”
Many other WFPB doctors extol the virtue of exercise, but they all consider that it must be within the context of a healthy plant-based diet.
Which does the science say is more important – diet or exercise?
In his book How Not To Die 8 , Dr Michael Greger makes it pretty clear that, whilst exercise is important, it’s diet that’s the biggie when it comes to warding off obesity and other chronic diseases:
“The food industries like to blame inactivity as the prime cause of obesity, not the promotion and consumption of their calorie-rich products 9 . On the contrary, however, research suggests that the level of physical activity may have actually increased in the United States over the past few decades 10 . We know that obesity is rising even in areas where people are exercising more 11 . This is likely explained by the fact that eating activity levels are outstripping physical activity levels 12 .
“Surveys suggest that most people believe controlling diet and getting enough exercise are equally important for weight control 13 . Researchers who accept grants from the Coca-Cola Company 14 call physical inactivity “the biggest public health problem of the 21st century.” 15 . Actually, physical inactivity ranks down at number five in terms of risk factors for death in the United States and number six in terms of risk factors for disability 16 . And inactivity barely makes the top ten globally 17 .
“…diet is by far our greatest killer, followed by smoking 16 . Of course, that doesn’t mean you should sit on the couch all day. As we’ve seen in this book, in addition to helping you enjoy a healthy body weight, exercise can also ward off and possibly reverse mild cognitive decline, boost your immune system, prevent and treat high blood pressure, and improve your mood and quality of sleep, among many other benefits.” 18
Which is more effective – exercise or drugs?
A 2013 BMJ review 19 concluded that: “Although limited in quantity, existing randomised trial evidence on exercise interventions suggests that exercise and many drug interventions are often potentially similar in terms of their mortality benefits in the secondary prevention of coronary heart disease, rehabilitation after stroke, treatment of heart failure, and prevention of diabetes.”
As pointed out by the PCRM website 20 this review, which analysed more than 305 trials with 339,274 participants, compared drug and exercise interventions and it found that: “…exercise proved similar to medications for heart disease prevention, heart failure treatment, and diabetes prevention. For those who had suffered a stroke, exercise was more effective than drug treatment. In addition, physical activity often provided patients with fewer side effects and injuries. The authors stress that these data provide health care professionals with a safe and effective alternative for their patients.”
What are some of the benefits of exercise?
Dr Greger considers that: “…in addition to helping you enjoy a healthy body weight, exercise can also ward off and possibly reverse mild cognitive decline, boost your immune system, prevent and treat high blood pressure, and improve your mood and quality of sleep, among many other benefits.” 18
The science certainly seems to support the importance of physical exercise for preventing/treating a whole range of chronic diseases affecting all parts of the body, including:
- the heart
- regular physical activity reduces the risk of coronary heart disease and diabetes by 30-50% 21
- when you exercise, the heart muscle gets a workout too. Over time, the heart becomes more efficient, allowing the resting heart rate to decrease—beneficial, since a high resting heart rate is a risk factor for cardiac mortality 22 23
- regular exercise helps to increase production of nitric oxide, a key regulator of blood pressure. In addition to reduced blood pressure, resulting in improved blood flow to skeletal muscle and the heart 24 25
- the brain
- physical exercise is a natural mood elevator, and has been shown to be just as effective as (and, naturally, much safer than) anti-depressant drugs 26 27 28 29
- physical activity has consistent and long links to cognitive abilities and mental alertness 30
- for older adults, regular walking was shown to decrease the risk of cognitive impairment 31 , and strength training also produces cognitive benefits 32
- the whole body
- muscle strength is regarded as the best predictor of bone strength— exercise protects against osteoporosis 33 34 35
- a decreased risk of colon, breast, and prostate cancers are associated with increased physical exercise, thought to partly due to the effects on the insulin-like growth factor 1 (IGF-1) system 36
- the body’s antioxidant defences are built and maintained by regular physical exercise 24
- sleep is enhanced by exercise 37 38
- exercise protects against chronic inflammation 39
Final thoughts
So, which is most important, then – exercise or diet? I think it’s clear from the above that both are important. However, if I was to recommend one rather than the other, it would be diet every time. There’s some benefit in exercising while still eating the toxic SAD (Standard American Diet) full of excess animal protein, fat and cholesterol, processed junk, salt, sugar and oils; but the benefit would be minimal compared with doing relatively no exercise but simultaneously eating a WFPB diet.
You couldn’t go far wrong if you simply followed Dr Greger’s Daily Dozen – treat exercise as one of the daily components of your optimal diet and lifestyle – the best of both worlds…

- Let’s Move Campaign – Michelle Obama. [↩]
- The Campbell Plan by Thomas Campbell, MD [↩]
- Reasons You Should Include Exercise in Your Diet Plan. March 27, 2015. By Thomas Campbell, MD. [↩]
- Dr. Greger’s Daily Dozen Checklist. Michael Greger M.D. FACLM September 11th, 2017 Volume 38 [↩]
- How Much Should You Exercise? Michael Greger M.D. FACLM April 28th, 2017 Volume 35 [↩]
- Exercise Has Surprising Benefits for Your Heart and Brain. May 21, 2016 by Joel Fuhrman, MD [↩]
- The End of Heart Disease by Joel Fuhrman [↩]
- How Not To Die by Dr Michael Greger [↩]
- Freedhoff Y, Hébert PC. Partnerships between health organizations and the food industry risk derailing public health nutrition. CMAJ. 2011;183( 3): 291– 2. [↩]
- Westerterp KR, Speakman JR. Physical activity energy expenditure has not declined since the 1980s and matches energy expenditures of wild mammals. Int J Obes (Lond). 2008;32( 8): 1256– 63. [↩]
- Dwyer-Lindgren L, Freedman G, Engell RE, et al. Prevalence of physical activity and obesity in US counties, 2001– 2011: a road map for action. Popul Health Metr. 2013;11: 7. [↩]
- Laskowski ER. The role of exercise in the treatment of obesity. PMR. 2012;4( 11): 840– 4. [↩]
- Matthews J, International Food Information Council Foundation. Food & Health Survey: Consumer Attitudes Toward Food Safety, Nutrition & Health. August 31, 2011. [↩]
- Archer E, Hand GA, Blair SN. Correction: Validity of U.S. Nutritional Surveillance: National Health and Nutrition Examination Survey Caloric Energy Intake Data, 1971– 2010. October 11, 2013. [↩]
- Blair SN. Physical inactivity: the biggest public health problem of the 21st century. Br J Sports Med. 2009;43( 1): 1– 2. [↩]
- Murray CJ, Atkinson C, Bhalla K, et al. The state of US health, 1990– 2010: burden of diseases, injuries, and risk factors. JAMA. 2013;310( 6): 591– 608. [↩] [↩]
- Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990– 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380( 9859): 2224– 60. [↩]
- Greger, Michael; Stone, Gene. How Not To Die: Discover the foods scientifically proven to prevent and reverse disease (Air Side Edt) (pp. 392-394). Pan Macmillan. Kindle Edition. [↩] [↩]
- Naci H, Ioannidis JPA. Comparative effectiveness of exercise and drug interventions on mortality outcomes: metaepidemiological study. BMJ. Published online October 1, 2013. [↩]
- PCRM: Exercise as Effective as Drugs in Disease Treatment. October 3, 2013. [↩]
- Bassuk SS, Manson JE. Epidemiological evidence for the role of physical activity in reducing risk of type 2 diabetes and cardiovascular disease. J Appl Physiol 2005;99:1193-1204. [↩]
- Duncker DJ, Bache RJ. Regulation of coronary blood flow during exercise. Physiol Rev 2008;88:1009-1086. [↩]
- Verrier RL, Tan A. Heart rate, autonomic markers, and cardiac mortality. Heart Rhythm 2009;6:S68-75. [↩]
- Kojda G, Hambrecht R. Molecular mechanisms of vascular adaptations to exercise. Physical activity as an effective antioxidant therapy? Cardiovasc Res 2005;67:187-197. [↩] [↩]
- Brown MD. Exercise and coronary vascular remodelling in the healthy heart. Exp Physiol 2003;88:645-658. [↩]
- Medina J: brain rules. . Seattle, WA: Pear Press; 2008.)) ((Hyman M: The UltraMind Solution. New York, NY: Scribner; 2009. [↩]
- Gill A, Womack R, Safranek S. Clinical Inquiries: Does exercise alleviate symptoms of depression? J Fam Pract2010;59:530-531. [↩]
- Uebelacker LA, Epstein-Lubow G, Gaudiano BA, et al. Hatha yoga for depression: critical review of the evidence for efficacy, plausible mechanisms of action, and directions for future research. J Psychiatr Pract 2010;16:22-33. [↩]
- Saeed SA, Antonacci DJ, Bloch RM. Exercise, yoga, and meditation for depressive and anxiety disorders. Am Fam Physician 2010;81:981-986. [↩]
- Medina J: brain rules. . Seattle, WA: Pear Press; 2008. [↩]
- Erickson KI, Raji CA, Lopez OL, et al. Physical activity predicts gray matter volume in late adulthood: the Cardiovascular Health Study. Neurology 2010;75:1415-1422. [↩]
- Davis JC, Marra CA, Beattie BL, et al. Sustained Cognitive and Economic Benefits of Resistance Training Among Community- Dwelling Senior Women: A 1-Year Follow-up Study of the Brain Power Study. Arch Intern Med2010;170:2036-2038. [↩]
- Arq Bras Endocrinol Metabol. 2014 Jul;58(5):514-22. Physical exercise and osteoporosis: effects of different types of exercises on bone and physical function of postmenopausal women. Moreira LD, Oliveira ML, Lirani-Galvão AP, Marin-Mio RV, Santos RN, Lazaretti-Castro M. [↩]
- Osteoporos Int. 2014 Aug;25(8):2017-25. doi: 10.1007/s00198-014-2724-3. Epub 2014 May 8. The effect of exercise and education on fear of falling in elderly women with osteoporosis and a history of vertebral fracture: results of a randomized controlled trial. Olsen CF1, Bergland A. [↩]
- Osteoporos Int. 2015 Oct;26(10):2491-9. doi: 10.1007/s00198-015-3165-3. Epub 2015 May 12. Exercise and fractures in postmenopausal women. Final results of the controlled Erlangen Fitness and Osteoporosis Prevention Study (EFOPS). Kemmler W, Bebenek M, Kohl M, von Stengel S. [↩]
- American Institute for Cancer Research: The Exercise Factor. [↩]
- Atkinson G, Davenne D. Relationships between sleep, physical activity and human health. Physiol Behav2007;90:229-235. [↩]
- Montgomery P, Dennis J. Physical exercise for sleep problems in adults aged 60+. Cochrane Database Syst Rev2002:CD003404. [↩]
- Mathur N, Pedersen BK. Exercise as a mean to control low-grade systemic inflammation. Mediators Inflamm2008;2008:109502. [↩]

 If the only reason you continue eating animal products is because of taste, then I can tell you that a no-SOS WFPB diet is really tasty and satisfying. Of course, you won’t believe it, but neither would a lot of vegans if they thought they had to give up their olive oil, fake ice-cream, fake sausages/burgers or white pasta.
If the only reason you continue eating animal products is because of taste, then I can tell you that a no-SOS WFPB diet is really tasty and satisfying. Of course, you won’t believe it, but neither would a lot of vegans if they thought they had to give up their olive oil, fake ice-cream, fake sausages/burgers or white pasta.












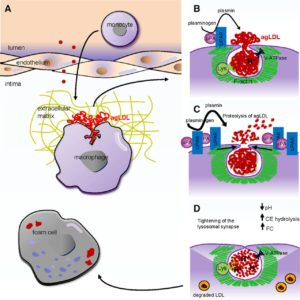
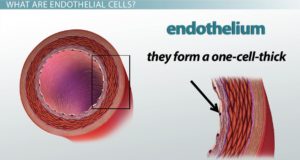 The endothelial cell layer is a one-cell thick layer within the inner surface of our blood vessels. These cells are of vital importance for vascular health and their damage is what leads to the development of CVD (cardiovascular disease).
The endothelial cell layer is a one-cell thick layer within the inner surface of our blood vessels. These cells are of vital importance for vascular health and their damage is what leads to the development of CVD (cardiovascular disease).