Okay, if you made bread from whole grains rather than floured grains, it would be a bit of a mess! However, there are compelling reasons why eating whole grains (wheat, barley, buckwheat, etc) provides far more health benefits than eating even the healthiest goods made with flour. And we’re not talking here about wholegrain, 1 as opposed to processed or refined grains – we’re talking about the whole grain – the complete edible part of the grain which has not been milled or ground down to millions of small particles, as happens when making any flour – be it wholegrain/wholemeal or highly refined (white flour).
The central message of this article concerns the different effects that grains and flours have inside your guts. First, though, a bit of background.
Blog Contents
Anatomy of a grain
The above diagram shows the three parts of a grain:
bran – the outer shell which protects the grain, containing most of the fibre
endosperm – the major internal part providing food (energy) to the germ
germ – the smaller internal part which provides the seed for future generations
What happens during flour milling?
When whole grains are milled to make refined flour, the bran and germ are removed, leaving only the endosperm. When whole grains are milled to make wholegrain flour, all three parts are ground down and made into a flour. Most people would have become aware that refined (white) flour is not as good for you as wholegrain flour, since the latter still provides some of the benefits of fibre, including:
helping to control blood glucose levels – thereby reducing sugar/insulin spikes
helping to maintain/ improve insulin resistance – a central feature of type 2 diabetes
increasing stool bulk – easing passage through the intestines and helping to prevent constipation
keeping you feeling full for longer
reducing blood cholesterol
Which grain has most fibre?
Just out of interest, the following is a list 2 of various grains, showing the average fibre content:
Take it out to put it back in
Vitamin E (a powerful antioxidant) 3 , B vitamins (essential for energy production, amongst other things) and trace minerals (including magnesium, selenium and zinc) 4 are partly destroyed by the time the final flour-based products have been baked. This is especially the case with ‘white’ flour (white because the darker-coloured fibre has been removed).
As an example, during milling, wheat loses 50% of its original phosphorus and calcium, 66% of iron, 50-70% of thiamine (vitamin B1)), 80% of niacin (vitamin B3), and 33% of tocopherol (vitamin E) 5 .
These and other nutrients – usually synthetic versions 6 – can then be added back into the final flour, thereby ‘enriching’ or ‘fortifying’ it. All well and good, but there’s plenty of strong evidence 7 suggesting, not only that the original nutrients combined within the actual plant (in this case, grains) are more effective than separately added vitamins and minerals, but studies 8 also show that some added ‘nutrients’ can be seriously harmful to health.
What else does commercially prepared flour contain?
I’m not even bothering to consider other flour products apart from bread (such as pies, pasties, cakes etc). The latter are generally so full of junk (whether animal- or plant-based) that, even if the pastry were of the highest possible quality, the product usually contains other ingredients than few WFPB nutritionists would recommend. However, if you’re determined to eat bread, the range of commercially produced offerings range from the reasonably okay to the downright awful.
“Dozens of similar studies demonstrate that if you reduce your salt intake, you may reduce your blood pressure. And the greater the reduction, the greater the benefit may be. But if you don’t cut down, chronic high salt intake can lead to a gradual increase in blood pressure throughout life.“
sugar
some of my recipes contain a small amount, but commercial breads usually contain far too much
“Research confirms that ingestion of oil, no matter which type of oil or whether it was fresh or deep fried, showed a significant and constant decrease in arterial function.” 12
“The bottom line is that there is no direct human data suggesting harm from eating GMOs, though in fairness such studies haven’t been done, which is exactly the point, critics counter. That’s why we need mandatory labelling on GMO products so that public health researchers can track whether GMOs are having any adverse effects.”
And this isn’t a definitive list..
There have to be some benefits of refined flour…
Whilst there are no obvious health benefits to stripping whole grains of bran and germ, it does provide a longer shelf life. It also means the products ‘hit the sweet spot’ more quickly and can be a lot more addictive. The producers and retailers benefit when the consumer can’t resist another slice (or two) of the easily chewed and digested pap. So what if the blood glucose hits the roof? It’s well-known that when blood sugar levels rise quickly, they’ll drop just as quickly and result in rebound hunger. Your hunger won’t leave you alone.
Whole grains and the microbiome
This is the take-home bit of the blog. When you eat a milled grain, which consists of millions of tiny particles, most of it gets absorbed and digested well before it reaches your large intestine (the colon). However, when you eat a whole grain, chewing and digestion in the stomach and small intestine tend to leave much larger ‘chunks’ of grain that reach the colon.
So what?
In the colon, trillions of gut bacteria (the microbiota or gut flora) are waiting for these chunks of grain (prebiotics) so that they can further digest them and, thereby, release bi-products back into our bloodstream – bi-products which are of significant importance to our overall health – from reinforcing our immune system, protecting the endothelial cells of our blood vessels, to protecting us from mental depression.
The fascinating subject of gut bacteria has been covered in great detail in several previous blogs 24252627 . The chunks of whole grain act as prebiotics for our gut bacteria.
Final thoughts
So, if you want to provide valuable fuel for those little guys down there in your colon, stick to whole grains (boiled first, of course), and leave the bread, pasties, cakes, biscuits and other flour products on the shelf for the most part.
If you can’t live without bread, try to make it yourself. I’ve provided some really simple recipes 282930 for a variety of bread types, each of which avoids the use of salt and oil. And if you can’t live without a bit of salt in your bread, then still best to make it yourself rather than buy commercially prepared bread.
References
Wholegrain, wholewheat and wholemeal are all terms which tend to be used interchangeably to refer to the same thing. [↩]
It could be argued that the major nutritional problem experienced by those of us in ‘developed’ countries is an excess of macronutrients (particularly animal protein, saturated fat and sugar) plus salt. When this is combined, as it usually is, with a corresponding insufficient intake of micronutrients (minerals, vitamins, fibre and phytonutrients from fruit, veg, grains, legumes, nuts and seeds), then one descends the slippery slope towards truly unpleasant diseases and a likely early death.
Blog Contents
Fatty under-nutrition
Whilst the term ‘over-nutrition’ is often used to define this modern dietary dilemma, it should really be thought of as ‘under-nutrition’, being that it’s too low in nutrients and too high in calories – a sort of nutrient starvation as the body expands. This is an utterly new paradox, probably never seen on this planet prior to the last few human generations.
When FUN is no fun
For the sake of clarity, I’m going to term this condition ‘Fatty Under-Nutrition’, or FUN for short.
The FUN starts young
The FUN starts early in life – even before birth. When women become pregnant, they’re usually urged to eat more because they’re “eating for two”, even though expectant and lactating mothers only require an additional 300 or so calories each day 1 . What all pregnant women really should watch is that they eat a healthy and varied diet, sufficient in macronutrients, but which includes all the micronutrients they and their baby need – notably, omega-3 fatty acids (DHA, in particular), iron, calcium, choline, iodine, vitamins C, D, B9 and, especially in the case of pregnant women eating a WFPB/vegan diet, plus sufficient vitamin B12 2 . Of course, any supplementation should always be in consultation with the medical professional (OB or GP) who is overseeing the pregnancy.
Excessive FUN, that is, a diet low in micronutrients but high in macronutrients (especially animal protein, saturated fat and sugar) during pregnancy can have a range of effects on the health of the mother and baby. The most obvious is excessively rapid weight gain in the mother. However, this factor alone has been shown 34 to:
increase the risk of labour induction
increase the risk of caesarean section
result in a higher birth weight
cause other complications during pregnancy and delivery
And it’s not just the mother
When infants and children are overfed, they can develop unhealthy dietary habits which may last a lifetime – being apparent in both their waistline and in the number of visits they need to make to their doctor and to the hospital later in life. Both quantity and type of food eaten in childhood can lead to metabolic implications with lifelong consequences.
Since mothers and expectant mothers want to do the very best for their children, they can be susceptible to over-feeding themselves and their babies in spite of their most loving and caring intentions. As one study stated: “In general, women are especially receptive to advice about diet and lifestyle before and during a pregnancy. This should be exploited to improve the health of future generations” 5 . Of course, in order to achieve this, the quality of the advice needs to be of the highest order.
In 2004, the American Dietetic Association pointed out that: “…the number of children who are overweight has more than doubled among 2- to 5-year-old children and more than tripled among 6- to 11-year-old children, which has major health consequences. This increase in childhood overweight has broadened the focus of dietary guidance to address children’s over consumption of energy-dense, nutrient-poor foods and beverages and physical activity patterns. Health promotion will help reduce diet-related risks of chronic degenerative diseases, such as cardiovascular disease, type 2 diabetes, cancer, obesity, and osteoporosis.” 6
A 2000 study stated that: “During early life and development the embryo, fetus and infant are relatively plastic in terms of metabolic function. The effect of any adverse environmental exposure is likely to be more marked than at later ages and the influence is more likely to exert a fundamental effect on the development of metabolic capacity” 7 . Whilst any baby, infant or young child faces health problems if they are significantly underweight, it’s increasingly understood that being overweight can be equally problematic – if not more so in some respects. 8910
A 2005 review 11 concluded that: “Infants who are at the highest end of the distribution for weight or body mass index or who grow rapidly during infancy are at increased risk of subsequent obesity.
A 2006 study 12 showed that when a 4-month infant is fed more calories than recommended, it is a strong predictor of both increased weight gain before 2 years and increased risk of becoming obese in childhood and adulthood.
The take-home message of this is that parents and care-givers should choose foods that promote a healthy body weight and resist the temptation to ‘spoil’ with food or aim to promote the rapid growth of their child through overfeeding.
Teen FUN
An increasing percentage of adolescents are now over-weight. As of 2018, around a third of UK children between 2 and 15 are clinically obese13 , and US childhood obesity has more than doubled in the past 25 years 14 . Increases in pre-diabetes and full-blown type 2 diabetes (T2D) in childhood is just one disease correlated with childhood obesity 15 . Unless dietary changes are made, T2D symptoms are likely to remain and increase as these young people pass into adulthood. This is made more probable by the fact that the medical professions are slow to change from viewing T2D as a life-long, irreversible condition – thereby their efforts are aimed at merely ‘managing’ the disease, rather than viewing it as a completely reversible condition if appropriate dietary and lifestyle changes are made and adhered to. 16
“Type 2 diabetes is rising rapidly in children and adolescents worldwide. Changing a child’s living environment to include physical activity, and a well balanced, low fat, high fiber diet, are important for the maintenance of a desirable body weight and improving insulin sensitivity…and decrease the risk of diabetes and cardiovascular disease.” 17
Fastest way to FUN
Just two words can sum up the major cause of FUN: ‘fast’ and ‘food’. Whether from take-aways, restaurants or supermarket shelves, fast food provides that perfect storm of high calories/low nutrients for children and adults alike.
One of the key findings of a 2018 study into fast food purchases for children by their parents in the US was:
“Parents’ purchases of fast food for their children have increased in recent years:
In 2016, 91% parents reported purchasing lunch or dinner for their child in the past week at one of the four largest fast-food restaurants, on average twice per week.
In contrast, 79% reported purchasing fast food for their child in the past week in 2010.” 18
As far back as 2003, a US report 19 indicated that fast-food use was reported by 42% of children, resulting in:
high intake of energy, fat, saturated fat, sodium, carbonated soft drinks, but
low intake of vitamins A and C, fruits and vegetables
FUN leads to yo-yo dieting
This problem becomes compounded when the adolescents try to lose weight by attempting various restrictive dieting regimes – most of which fail and many of which exacerbate existing and/or create new health problems.
“Cross-sectional and prospective surveys have shown that a large percentage of adolescents, particularly females and even those of normal weight, diet at some time. While moderate changes in diet and exercise have been shown to be safe, significant psychologic and physiologic consequences may occur with extreme or unhealthy dieting practices. Moderate dieting has been shown to be associated with negative self-esteem in some adolescents. The very act of starting any diet increases the risk of eating disorders in adolescent girls. Extreme methods of weight loss can have adverse physiologic effects if not closely monitored. Electrolyte disturbances, cardiac dysrhythmias, and even sudden cardiac death can result from unhealthy or extreme dieting practices. Such practices are associated with other problem behavior in adolescents.” 20 .
A 2016 study 21 reported that, at any given time, more than 25% of male and around 60% of female adolescents are dieting in order to lose weight. In addition, up to 9% reported that they use maladaptive dieting habits, such as purging22 .
Developing FUN in adulthood
It’s in so-called ‘developed’ countries that both children and adults are at particular risk from FUN.
Whilst a significant proportion (around 50%) of North Americans have inadequate intake of essential micronutrients and fibre, their energy balance is usually far in excess of physiological needs. And it’s been known for some time that adults shouldn’t only be worried about this FUN leading to obesity and T2D:
“Diet is estimated to contribute to about one-third of preventable cancers — about the same amount as smoking. Inadequate intake of essential vitamins and minerals might explain the epidemiological findings that people who eat only small amounts of fruits and vegetables have an increased risk of developing cancer. Recent experimental evidence indicates that vitamin and mineral deficiencies can lead to DNA damage.” 23
Energy density, portion size & availability
Standard foods, such as dairy, meat, sugar and vegetable oils tend to be more energy-dense in modern Western diets (often referred to as the SAD – Standard American Diet) when compared with the more traditional Asian and African diets, in which grains, legumes, and starchy vegetables play a much larger part.
Add to this the fact that, in Western societies, food portion sizes are larger and calorie dense/nutrient poor foods are much more easily available, and you have an adult population experiencing epidemic obesity-related diseases: coronary heart disease, hypertension, diabetes, and cancer. 24
FUN into old age – if you last that long…
As our populations reach advanced age, metabolic syndrome25 is becoming the norm rather than the exception, with more than 40% of people in their 60’s and 70’s being affected 26 and, thereby, running a greater risk of dying prematurely 27 .
And dying isn’t even the worst of it. These chronic illnesses, during later years of one’s life, require regular hospitalisation, invasive, painful, and often humiliating medical procedures, restrictions of one’s privacy and independence, and severe limitations on the quality and enjoyment of one’s wise elderly years – years that should be active, happy and golden.
When the FUN stops
When you choose to eat a balanced WFPB diet, the FUN stops and the fun begins. Nutrient-rich foods become the norm and both micronutrients and macronutrients take care of themselves, with the ideal ratio of protein, fat and carbohydrate already wrapped up by nature with all the vitamins, minerals, phytochemicals and fibre that your body needs.
And no longer will you have to restrict how much you eat, nor worry about your weight, another paradox – albeit a very welcome one! – since, with such naturally healthy eating, you can’t help but get back to your ideal weight, thereby obviating the risk of falling into the cycle of yo-yo dieting.
Naturally, you’ll still be strongly advised to take B12 supplements and ensure you get enough sunlight, or else take vitamin D supplements; but apart from this, you can just concentrate on enjoying the rest of your life while your body and mind are naturally fuelled for optimal performance.
And all this by simply eating unadulterated plant foods…
Purging – a practice known as bulimia – oscillates with bingeing and can result in a wide range of health issues, including rupture of the oesophagus or stomach, dental and oral damage due to stomach acid exposing during vomiting. [↩]
Metabolic syndrome is a combination of central obesity, dysglycaemia, dyslipidemia and arterial hypertension. Most of the disorders associated with metabolic syndrome have no visible symptoms except for a large waist circumference. Additional symptoms include increased thirst and urination, fatigue, and blurred vision. [↩]
Increased appetite is a driving force for weight gain, and unchecked weight gain does, of course, lead to obesity. There’s a growing body of literature suggesting that ghrelin, the so-called “hunger hormone” or “starvation hormone”, plays an important role in appetite fluctuations. Whilst we looked at leptin, the “satiety hormone” in the previous blog 1 , this one is an analysis of some research on ghrelin and obesity 2 .
Because this is a rather complex blog, technical terms are in green – either click associated number to go to References/Notes section (blue arrow returns to same place in the text), or hold cursor over relevant number to reveal contents.
Blog Contents
What is ghrelin?
The complexity of this topic starts as soon as one looks for the derivation of the word “ghrelin”, with some authorities 3 stating that it’s derived from “ghre” (grow) and “relin” (release), while another authorities4 appear to relate its etymological roots to the use of letters from its understanding as a “Growth Hormone RELease INducing” hormone. In any case, it is agreed that it was first isolated and identified by Kojima and Kangawa et al in 1999 5 . Three years later, its specific brain receptor, GHS-R 1a, was also identified 6 .
Whilst leptin is mainly secreted by fat cells 7 and insulin is secreted by beta cells in the islets of Langerhans within the pancreas, ghrelin is primarily secreted from cells in the stomach (see below for more detail on this).
Ghrelin vs leptin
Having already looked at leptin in the previous blog, it’s worth starting by drawing comparisons between it and ghrelin, since they are regarded as working together (although in opposite directions) to help regulate appetite and metabolism.
Ghrelin and leptin are the two hormones8 that are most responsible for regulating appetite – to ensure you don’t eat too few calories and starve to death while also ensuring you don’t eat too many calories and become obese. Well, that’s the hope anyway!
As an appetite stimulant, ghrelin is called an orexigenichormone9 that stimulates food intake and thereby helps regulate body weight, while the appetite-inhibiting hormone leptin is known as an anorexigenichormone10
They are both homeostatic11 hormones which means they are going to act on the hypothalamus12 , the part of the brain that maintains the body’s internal balance (homeostasis).
The hypothalamus acts as the link between the endocrine13 and nervous14 systems. The hypothalamus produces releasing and inhibiting hormones, which stop and start the production of other hormones throughout the body.
Ghrelin and leptin act on different parts (receptors) within the hypothalamus.
Ghrelin acts on the lateral15 hypothalamic brain cells16 , while leptin acts on the ventromedial17 hypothalamic brain cells.
“Ghrelin makes you Grow” – makes you eat, while “Leptin makes you Lean” – makes you stop eating. These are two mnemonics that might help to remember which is which.
Ghrelin is the only peripheral18 orexigenic hormone that activates receptors found in the appetite centre – viz. the hypothalamus and pituitary gland.
Ghrelin is produced by endocrine cells 19 of the oxyntic glands20 within the gastricfundus21 . It’s also secreted, to a lesser extent, by the body of the stomach, the mucosa of the duodenum and jejunum22 , the lungs, the urogenital organs, and the pituitary gland.
Stomach distension reducing ghrelin-production and inhibiting appetite.
Once produced in the stomach, ghrelin is released into the bloodstream, passes through the blood-brain-barrier23 to the lateral hypothalamus, and causes a hunger response.
Ghrelin will also have an effect on the stomach itself, causing an increase in gastric acid production and gastric motility 24 . This prepares the stomach for the food that’s been anticipated by the brain. Daily habits (breakfast, lunch and dinner) become ingrained so that our ghrelin production starts to increase before we’re even consciously aware that we’re hungry.
Ghrelin stimulants (or inducers) include hypoglycaemia (low blood glucose), an empty stomach, and low body weight (low body fat content).
Ghrelin suppressants (or inhibitors) include activation of the stomach’s stretch receptors as the stomach becomes full of food (stomach distension).
Leptin, on the other hand, is primarily produced by white adipose tissue.
As the fat cells increase in size, they produce more leptin. A negative feedback signal 25 is caused when leptin travels from the fat cells, through the bloodstream and blood-brain-barrier to the ventromedial hypothalamic cells in the hypothalamus – reducing appetite and food intake. Ideally, this means that fat controls its own levels within the body. 26
Inducers for leptin include insulin and emotional stress. Below, we consider how modern dietary changes may have messed with the normally healthy relationship between stress and hunger hormones.
Leptin and insulin share common effects in controlling food intake and energy metabolism, with each playing an important role in blood glucose homeostasis. They directly regulate each other: leptin inhibits insulin and insulin stimulates leptin synthesis and secretion.
Note: ANS = Autonomic Nervous System.
Leptin increases insulin sensitivity 27 , in part, by decreasing adiposity and lipotoxicity28 . Leptin decreases hepatic (liver) production of glucose – glycogenolysis29 – contributing to its glucose-lowering effects. 30
Studies have revealed that leptin has the effect of normalising hyperglycaemia31 and hyperinsulinaemia32 . It’s also clear 33 that levels of both need to drop for fat burning – i.e. gluconeogenesis34 – to commence.
Whilst it would seem intuitively obvious in evolutionary terms that when the body is under stress (fight or flight), appetite for food would be switched off – perhaps causing the production of leptin to achieve this, studies 35 have pointed out a complication in the modern world with psychological stress: namely, that it often results in “comfort eating” (usually fatty, sweet, high calories foods). The latter modern habit can confuse the picture.
The previous blog pointed 1 out the paradox that obese humans tend to have higher levels of leptin – the hunger-inhibiting hormone – suggesting they have developed leptin resistance. This results in a toxic cycle of increased leptin insensitivity leading to increased leptin levels (irrespective of insulin and ghrelin levels) leading to increased amounts of fat being stored in the body, leading to the fat cells producing even more leptin.
To test the latter, researchers intravenously increased leptin levels during times of emotional stress in order to see whether this would lower the compensatory intake of such comfort food. They concluded that “…initial findings suggest that acute changes in leptin [i.e. increasing it in the short term] may be one of the factors modulating down [reducing] the consumption of comfort food following stress.” 36
A major inhibitor of leptin is short term fasting. When you haven’t eaten for several hours, leptin levels should drop and ghrelin levels should rise. A theory which appears to work okay in healthy, non-obese individuals.
Active & inactive ghrelin
The acylation of inactive (non-acyl) to active (acyl) ghrelin.
There are several different forms of ghrelin, but the main two are called the “inactive” (des-acyl ghrelin) and “active” (acyl ghrelin – a peptide of 28 amino acids) forms. The inactive form accounts for more than 90% circulating within the bloodstream 37 . However, the inactive form has to be converted into the active form in order to do its work as an appetite stimulant. It does this via an enzyme called ghrelin O-acyltransferase or GOAT 3839 . This process is critical both for the orexigenic and the gastric-emptying actions of ghrelin.
How ghrelin exerts its effect on the body
There are various possible actions by which ghrelin exerts its effect within the body, including:
overproduction/underproduction of ghrelin before and/or after meals
increased/decreased receptor sensitivity to ghrelin action
Ghrelin & positive feedback
The appetite-generating effect of ghrelin can be described as a direct positive feedback loop40 which maintains increased activity of AgRP neurons41 so as to drive feeding behaviour until satiety is reached 42 , when leptin kicks in to do its job of suppressing appetite.
Other physiological functions of ghrelin
The discovery of the GOAT enzyme revealed that ghrelin is involved in many additional physiological functions, ranging from regulation of the immune and cardiovascular systems, up-regulation of insulin-like growth factor (IGF-1), to a dominant role in the gastrointestinal system and involvement in gastric emptying and intestinal motility43 .
Although it has a role as a growth factor secretagogue44 , stomach-derived ghrelin doesn’t appear to be necessary for growth and appetite stimulation, since ghrelin-deficient animals still appear to grow and eat quite normally 45 .
There must, therefore, be some form of redundancy within the body – that is, other physiological processes that promote growth and appetite which are able to compensate for the absence of ghrelin.
Actions and therapeutic pathways of ghrelin for gastrointestinal disorders
As can be seen in the diagram, ghrelin affects multiple systems. Whilst being secreted mainly by the stomach, it has effects in multiple areas, including the CNS (central nervous system), the immune system, the adrenal gland and the cardiovascular system. It can also affect the proliferation of osteoblasts 46 and neoplastic cells47 .
Ghrelin, obesity & appetite
The precise role of ghrelin in the pathophysiology of obesity is still under investigation. It’s considered by some that if we’re able to get a firm grip on how ghrelin initiates appetite, then increasing its level could be a revolutionary new method of obesity management and treatment.
The role of ghrelin in the development of obesity.
Reduced postprandial suppression of ghrelin in obese individuals
In a number of studies of obese adults and obese children 4849 , it’s been reported that postprandial suppression of ghrelin is lower in such obese groups compared to controls with normal body mass index (BMI).
This makes it a reasonable assumption that higher consumption of food by obese individuals is linked to a continuing feeling of hunger, even after consuming a meal with sufficient caloric content to satisfy their physiological needs. These findings have supported the ‘disease pattern’ of obesity which has underlying mechanisms and causes like other common disorders.
What’s the problem with ghrelin in relation to obesity?
So, is the obesity-ghrelin problem (and, by inference, the insulin-ghrelin problem) a matter of an overproduction of ghrelin or is it similar to what we’ve seen with leptin and insulin – i.e. insensitivity leading to resistance?
Since studies (mentioned above) 45 have shown that animals completely deficient in ghrelin can still grow normally without becoming obese, it would seem that the likeliest problem is the overproduction of ghrelin (regardless of the how much food is consumed) rather than a ghrelin insensitivity or oversensitivity. Various studies support this hypothesis 505152 , although uncertainty still remains regarding the precise mechanism/s involved, which range from a possible dysfunction in the gene for ghrelin to the production of antibodies to the peptide receptors which antagonise53 ghrelin’s effects which, in turn, might lead to disturbances in the production and actions of ghrelin. Additionally, interactions with other hormones (insulin, growth hormone (GH), etc) are likely to account for at least some of the ghrelin-obesity anomalies.
We still don’t fully understand the relationship between ghrelin and insulin – a relationship which appears to be based on an overproduction of ghrelin leading to a similar overproduction and eventual insensitivity/resistance to insulin 54 .
The view that the obesity-ghrelin problem is not due to an overproduction of ghrelin in obese individuals is supported by many studies. showing that the mean serum ghrelin level is generally lower in obese patients compared to lean individuals 5556 , although the number of ghrelin-producing cells was found to be more abundant in the fundus of morbidly obese patients.
You’d be excused for expecting obese individuals to have lots more of this appetite-promoting hormone floating around their bloodstream than would non-obese individuals, given that the former continue eating beyond their physiological needs. And you wouldn’t be alone. The following graph 57 reveals that, though ghrelin levels rise in expectation of a meal and fall after that meal in both obese and non-obese individuals, the levels of ghrelin are consistently higher in non-obese than in obese individuals.
A further study concluded: “Contrary to our hypothesis, however, obese subjects have lower plasma concentrations of the adipogenic58hormone ghrelin than age-matched lean control subjects.” 59
The same study made some suggestion about what’s actually happening with ghrelin in obese individuals, suggesting that it may be a downregulation60 of ghrelin as a consequence of elevated insulin or leptin, because fasting plasma ghrelin levels are negatively correlated with fasting plasma levels of insulin and leptin.
They also speculated that decreased secretion of ghrelin could be responsible for decreased levels of circulating growth hormone (GH) 61 in obese individuals 62 .
Ghrelin, growth hormone (GH), diabetes & obesity
Ghrelin, as stated above, causes the release of growth hormone (hence the proposed origin of its name – Growth Hormone Release Inducing hormone). The relationships between obesity, adipose tissue, GH and ghrelin make an already complex situation even more complex.
Obesity induces hyperinsulinaemia,hypoadiponectinaemia63 , hyperleptinaemia64 , reduced serum ghrelin, and increased free fatty acid levels. The effect of this is that GH secretion from the pituitary gland is suppressed 65 .
But what’s the relationship between low levels of GH and ghrelin in obese/diabetic individuals?
Insulin resistance is highly associated with visceral obesity, non-alcoholic liver disease, and type 2 diabetes. In turn, all these conditions are associated with low GH secretion. Since high levels of GH are likely to contribute to the development of insulin resistance when, that is, caloric intake is greater than physiological demand (when you eat more calories than you burn), the body’s reduction in GH secretion in obesity may be an adaptive phenomenon which is aimed at preventing insulin resistance occurring.
However, a problem occurs with this situation: namely, when GH secretion is reduced, it’s likely to lead to further increases in fat accumulation by reducing the process of lipolysis66 . It’s clear to see how this increased retention of fat can exacerbate obesity and establish a dangerous vicious circle. Indeed, truncal adiposity67 is one of the most important clinical findings of a condition known as adult GH deficiency syndrome (GHD) 68 .
So, when levels of circulating GH are reduced, as they are in cases of obesity, it’s proposed 59 that decreased plasma ghrelin concentrations – which are seen in obesity – represent a physiological adaptation to the positive energy balance69 associated with this disease.
GH (like insulin) is essential in adapting the utilisation of calories to the amount of ingested food, promoting anabolism70 in the case of positive energy balance, with catabolism71 occurring in the case of negative energy balance 72 . While insulin is the main metabolic hormone in the fed state (positive energy balance), GH assumes a key role as stimulator of lipolysis during prolonged fasting (negative energy balance), when it causes preferential oxidation of lipids and protein synthesis 73 .
“The increase in GH secretion that occurs with fasting may have represented an evolutionary advantage in times of food scarcity. However, GH and IGF-I have opposite effects on glucose homeostasis, with the former reducing insulin sensitivity (mainly acting in the liver) and the latter increasing it in the muscle.” 74
Plenty more detail on the relationship of ghrelin and GH is available in a number of excellent studies 75 .
Ghrelin and diets
As you’d expect, levels of ghrelin increase during dieting. This could explain why it’s very difficult to achieve long-term success from dieting. 7677
Two way to manage obesity
There are two main approaches in managing obesity:
conservative – e.g. diet, exercise and lifestyle changes
surgical – through various weight-loss surgical procedures, widely known as bariatric surgery
The conservative ways of preventing and treating diabetes, primarily through dietary changes, have been covered in such detail in previous blogs 78798081 that we hardly need to repeat them here.
Ghrelin & bariatric surgery
It’s clear that bariatric surgery is going to cause some purely mechanical effects (less room for food) that would be responsible for subsequent increased food restriction, as well as often leading to malabsorption82 . After all, the person concerned has had bits of their guts removed and/or joined together. However, during the past couple of decades, the identification of significant humoural83 changes (that lead to less hunger or earlier satiety postprandially) has complicated the picture of why appetite changes occur after such surgical procedures 8448 .
Ghrelin & two types of bariatric surgery
Researchers have recently tried to explain the impressive results of bariatric surgery in terms of weight loss by evaluating the changes in ghrelin concentration following roux-en-y gastric bypass (RYGB)85 and especially sleeve gastrectomy (SG)86 . In the latter procedure, the gastric fundus, where most ghrelin is produced, is totally removed. A recent meta-analysis 51 showed that the ghrelin level does fall significantly following SG. In patients who undergo RYGB, the results of various studies are contradictory 87 .
Does bariatric surgery work?
Both these techniques lead to exceptionally good results in weight loss. Based on the fact that, anatomically, SG is purely restrictive compared to RYGB, which additionally creates malabsorption by the rapid shunt of undigested food to the distal small intestine88 , the role of ghrelin is now being investigated more than ever. Whether or not bariatric surgery works, we know that even morbidly obese individuals can return to a normal healthy weight without the need for such extreme dietary measures 89 . Additionally, once the body is back to a healthy homeostatic state, one would assume that ghrelin levels would also normalise.
Ghrelin & age-related obesity
The adjacent graph 90 shows that ghrelin levels decrease with age, backed up by other studies 91 . This would be in line with the fact that ageing is accompanied by a decrease in both energy expenditure and locomotor activity – with decreases in muscle strength and endurance leading to functional decline. The latter factors, taken in isolation, would imply that there would be a corresponding increase in body weight, particularly in the form of fat.
This has an effect on food intake as well as energy expenditure, thereby potentially preventing the development of age-related obesity. 92
Ghrelin and anorexia
Due to the proven relationship of ghrelin with appetite, researchers are also investigating the potential connection of ghrelin to anorexia. Insight into the modification of the endogenous ghrelin system seems to be promising not only for the control of obesity, but also for the management of clinically significant anorexia and pathological weight reduction.
Does anorexia produce ghrelin insensitivity?
Accumulating evidence has shown that in patients with anorexia nervosa, there’s a paradoxical increase in plasma ghrelin level even when compared with matched controls or obese patients 93 , suggesting that the situation may be one of ghrelin-insensitivity 94 .
Ghrelin – homeostatic and non-homeostatic feeding
Anorexia nervosa, bulimia nervosa95 and other eating disorders appear to have pathophysiologies96 linked to dysfunctions of reward mechanisms. 97 Additional research 98 supports the hypothesis that ghrelin doesn’t just increase appetite by homeostatic need – that is, feeding driven by a metabolic need where hormones “speak to one another” in order to create homeostatic balance, but also by non-homeostatic feeding – that is, feeding driven by non-metabolic factors, such as reward (“hedonic feeding” 99 ) and memory. The latter factors have less to do with the body trying to reach homeostatic balance than with emotional, psychological and social factors.
Tail wagging the dog
The huge increase in the consumption of ultra-processed foods (high in sugar/fat/calories and low in nutrients) could be regarded as a causal factor in the dysregulation of homeostatic hormonal systems (ghrelin, leptin, insulin, etc), resulting in the tail (learned emotional need) wagging the dog (actual physiological need). This results in our medical professions struggling to cope with the ever-increasing effects of diet-related diseases, and in millions of suffering people who end up with diseased bodies and shortened lives.
Cancer and ghrelin administration
Ghrelin and cancer.
In vitro studies 100 have documented that both intra-peritoneal 101 and systemic102 administration of ghrelin have the potential of improving appetite and nutritional status, and at the same time reducing the metabolic rate in patients with end-stage cancer.
This research suggests a likelihood that additional gastric disorders (e.g. gastritis, GI tract carcinoma, and other functional GI disorders) disrupt the morphological structure103 of the stomach, and thus alter ghrelin production – being that the stomach is its major source. “These alterations may induce various GI disorders including functional GI disorders, eating disorders, abnormal energy homeostasis and growth. By understanding ghrelin secretion in the regulation of GI disorders, ghrelin levels may serve as a good diagnostic biomarker for early detection of GI disorders.” 100
The roles that ghrelin may play in relation to cancer is still relatively unclear. One study concludes: “It is currently unclear whether the ghrelin axis has tumor-promoting effects, or indeed whether it may inhibit tumorigenesis in vivo, and further studies are therefore required to elucidate its role in cancer.” 104
Limitations of Studies Investigating Ghrelin
There are several limitations in investigating ghrelin:
very small number of studies and RCTs (randomised controlled trials)
there are two forms of circulating ghrelin, inactive ghrelin (90%), and active acylated ghrelin (10%) 50 and published studies tending to measure total rather than active ghrelin levels
the active form of ghrelin has been reported to be unstable at room temperature
there’s a current lack of standardisation in ghrelin measurement in terms of timing of sample collection, collection method, follow-up period, sample storage, and the radioimmunoassays 105 being used
The latter issues make precise measurement a challenge and this may be an issue in the reproducibility of results in the future.
Prader-Willi syndrome (PWS)
PWS, a congenital form of obesity, is caused by a mutation on chromosome 15. One of the effects of this is that ghrelin levels are hugely increased and the individual is forever hungry. If untreated, eating far, far too much – resulting in morbid obesity. It’s thought 106 that elevated ghrelin levels in PWS children precede the onset of obesity.
Prader-Willi syndrome.
Prader-Willi syndrome vs non-congenital obesity
When ghrelin levels were compared between children with PWS and children with non-congenital obesity (i.e. nothing wrong with their chromosome 15), it was found 107 that, even immediately after eating meals, ghrelin levels remained comparatively much more elevated in the PWS children.
The reason for this is speculated 108 to be that hyperghrelinaemia109 in early infancy might be a response to the failure to thrive, and that chronic or persistent hyperghrelinaemia eventually promotes hyperphagia (overeating) in early childhood. 110
Once again, it would appear that more complexity has befallen us, since the obesity in PWS individuals is accompanied by elevated levels of ghrelin in the blood, while in non-congenitally obese individuals, ghrelin levels appear to be reduced even compared with non-obese individuals.
Further research on ghrelin
Whilst ghrelin research is ongoing, and all will hopefully be made clearer in the near future, a two-part YouTube video 111112 presents a very detailed analysis of the discovery of ghrelin and its receptor, along with its relationship to GH and its role in starvation-prevention.
Final thoughts
The above is by no means a comprehensive analysis either of the specific role/s of ghrelin in the development of obesity nor of its other varied physiological roles. Indeed, I haven’t even touched on another important appetite-suppressing hormone, namely PYY113 . Its relationship with ghrelin and other hormones is sufficiently complex to warrant a separate analysis, although there are plenty of studies for the interested reader. 114115116
What is clear, though, is that ghrelin appears to be attracting attention with regard to the treatment of obesity.
However, it does continue to be a source of irritation that, within the realm of medical research, so much emphasis is directed towards treatment (usually through searches for pharmaceutical and/or gene-based solutions) rather than prevention. And, as strong evidence suggests, obesity is best treated through dietary change; with the most effective and long-lasting dietary change being one that increases the ratio of whole plant foods to processed and/or animal foods 117118119 .
My expectation is that most research dollars will be spent on developing highly-profitable pharmaceutical solutions for perceived problems that relate to ghrelin and associated hormones. The elephant in the room is dietary change, of course. When we looked at toxic hunger vs real hunger 120 , we merely touched on the issue of ghrelin. However, it would seem relevant to this discussion to consider that eating a WFPB diet – which has significant impact on both homeostatic (the physiological effects of hormones, etc) and non-homeostatic feeding (‘comfort eating’ and ‘addictive’ dietary habits) – would also have direct and/or indirect effects on the effectiveness of the ghrelin-leptin-insulin-GH axis. Once again, more research is needed in this area, although where the research dollars come for this type of research is likely to be an ongoing problem.
Leptin is mainly secreted by adipocytes (fat cells) of white adipose tissue. It’s also produced in brown adipose tissue, placenta syncytiotrophoblasts, ovaries, skeletal muscle, the lower part of the fundic glands within the stomach, mammary epithelial cells, bone marrow, gastric chief cells and P/D1 cells. [↩]
A hormone is any member of a class of signalling molecules produced by glands in multicellular organisms that are transported by the circulatory system to target distant organs to regulate physiology and behaviour. [↩]
Orexigenic – An orexigenic, or appetite stimulant, is a drug, hormone, or compound that increases appetite and may induce hyperphagia – overeating. This can be a naturally occurring neuropeptide hormone such as ghrelin, orexin or neuropeptide Y, or a medication which increases hunger and therefore enhances food consumption. [↩]
Anorexigenic – an anorexigenic hormone reduces or inhibits appetite. [↩]
Homeostasis is the state of steady internal conditions maintained by living things. This dynamic state of equilibrium is the condition of optimal functioning for the organism and includes many variables, such as body temperature, fluid balance, blood sugar levels, and body weight being kept within certain pre-set limits. [↩]
The hypothalamus is an endocrine gland. Endocrine glands within the endocrine system secrete their products, hormones, directly into the blood rather than through a duct. The major glands of the endocrine system include the pineal gland, pituitary gland, pancreas, ovaries, testes, thyroid gland, parathyroid gland, adrenal glands and, of course, the hypothalamus. [↩]
The endocrine system is a chemical messenger system consisting of hormones, the group of glands of an organism that secrete those hormones directly into the circulatory system to regulate the function of distant target organs, and the feedback loops which modulate hormone release so that homeostasis is maintained. [↩]
The nervous system is the part of an animal that coordinates its actions by transmitting signals to and from different parts of its body. The nervous system detects environmental changes that impact the body, then works in tandem with the endocrine system to respond to such events. [↩]
Lateral means of, at, towards, or from the side or sides. The green cells on the diagram. [↩]
specifically, on the cell receptor known as the ghrelin/growth hormone secretagogue receptor or GHS-R. Secretagogue receptors are those that promote secretion. [↩]
Ventral means on or relating to the underside of an animal, plant or object – in this case the brain; while ventromedial indicates that it’s situated towards the middle of the ventral part. The red cells on the diagram. [↩]
Peripheral – that is, produced or taking place outside of the central nervous system , CNS – i.e. outside the brain and spinal cord [↩]
Oxyntic glands – these are made up of secretory cells which produce hydrochloric acid in the main part of the stomach, or the glands which they compose [↩]
the upper part of the stomach, which forms a bulge above the level of the opening of the oesophagus, furthest from the pylorus [↩]
Duodenum and jejunum are the first and second parts of small intestine, with the ileum being the final part before entering the large intestine, the colon. [↩]
The blood-brain barrier is a semipermeable membrane separating the blood from the cerebrospinal fluid, and constituting a barrier to the passage of cells, particles, and large molecules. Only specific substances, including ghrelin, are able to pass through this barrier. [↩]
Gastric or gastrointestinal motility is defined by the movements of the digestive system, and the transit of the contents within it. [↩]
A negative feedback (or balancing feedback) signal occurs when some function of the output of a system, process, or mechanism is fed back in a manner that tends to reduce the fluctuations in the output, whether caused by changes in the input or by other disturbances. [↩]
Lipotoxicity is a metabolic syndrome that results from the accumulation of lipid intermediates in non-adipose tissue, leading to cellular dysfunction and death. The tissues normally affected include the kidneys, liver, heart and skeletal muscle. [↩]
Glycogenolysis is the breakdown of the molecule glycogen into glucose, a simple sugar that the body uses to produce energy. The opposite of glycogenolysis is glycogenesis, which is the formation of glycogen from molecules of glucose. [↩]
Hyperglycaemia is an excess of glucose in the bloodstream, often associated with type 2 diabetes, also known as diabetes mellitus. [↩]
Hyperinsulinaemia is a condition in which there are excess levels of insulin circulating in the blood relative to the level of glucose. While it is often mistaken for diabetes or hyperglycaemia, hyperinsulinemia can result from a variety of metabolic diseases and conditions. [↩]
Gluconeogenesis is is a metabolic pathway that results in the generation of glucose, to be burned as energy, from certain non-carbohydrate carbon substrates, including fat and protein. [↩]
GOAT is essential for ghrelin-mediated elevation of GH, necessary to prevent death from severe calorie restriction through preservation of blood glucose levels. [↩]
Positive Feedback – a physiological cyclic process or action that can continue to amplify the body’s response to a stimulus until a negative feedback response, its opposite, takes over. [↩]
AgRP neurons – brain neurons that make agouti-related peptides – hence AgRP – that potently stimulate food intake [↩]
Intestinal mobility is the movements of the digestive system, and the transit of the contents within it. [↩]
A secretagogue is a substance that stimulates secretion of another substance – in this case, ghrelin stimulates the release of growth factor (GH) from the pituitary gland. [↩]
Osteoblasts are the cells required for bone synthesis and mineralisation, both during the initial formation of bone and during bone remodelling. [↩]
A neoplasm is an abnormal new growth of cells. The cells in a neoplasm usually grow more rapidly than normal cells and will continue to grow if not treated. [↩]
Adipogenesis is the formation of adipocytes (fat cells) from undifferentiated fibroblasts (preadipocytes). Fibroblasts are cells that are responsible for producing connective tissues in the body. [↩]
Downregulation is the process of reducing or suppressing a response to a stimulus. In this case, it’s a reduction in a cellular responses to ghrelin molecules due to changes in the number of activity of receptors. [↩]
Growth hormone is released from the pituitary gland to cause growth in children and affects bone density, lipid metabolism, and muscle in children and adults, stimulating amino acid uptake and protein synthesis in muscle and other tissues. Because a major role of growth hormone is to to stimulate the liver and other tissues to secrete IGF-1, this can be a problem if too much IGF-1 is produced in adults. Due to its insulin-like properties, IGF-1 can have serious and potentially fatal health effects including: diabetic (hypoglycaemic) coma, heart palpitations (tachycardia), facial nerve pain or paralysis (Bells Palsy), swelling of the hands, and so forth. [↩]
Hypoadiponectinaemia is characterised by low plasma adiponectin levels – a protein hormone that is produced by fat cells. Its physiological effects include the reduction of inflammation and atherogenesis (the formation of fatty deposits in the arteries) and enhancement of the response of cells to insulin. [↩]
Hyperleptinaemia is the presence of a higher than normal amount of leptin in the bloodstream. [↩]
Lipolysis is the breakdown of lipids and involves hydrolysis of triglycerides into glycerol and free fatty acids. It mainly occurs in adipose tissue, and is used to mobilise stored energy during fasting or exercise. [↩]
Truncal adiposity refers to obesity – fat retention – around the trunk of the body. [↩]
Positive energy balance occurs when the intake of food is greater than the output of work (as in muscular or secretory activity). The result is that the body stores extra food as fats. Negative energy balance occurs when the body draws on stored fat to provide energy for work. [↩]
Anabolism is a process a process that involves the synthesis of complex molecules from simpler molecules. These processes produce growth and differentiation of cells and increases in body size. Examples of anabolic processes include the growth and mineralisation of bone and increases in muscle mass. [↩]
Catabolism is the set of metabolic pathways that breaks down molecules into smaller units that are either oxidised to release energy or used in other anabolic reactions. [↩]
Negative energy balance is when energy demands exceed caloric supply – the opposite of positive energy balance. [↩]
Malabsorption occurs when the small intestine can’t absorb enough of certain nutrients and fluids – including macronutrients – proteins, carbohydrates, and fats – and micronutrients – vitamins and minerals – or both [↩]
relating to the body fluids, especially with regard to immune responses involving antibodies in body fluids as distinct from cells [↩]
Roux-en-y gastric bypass (RYGB) – from César Roux, the surgeon who first described it – a form of anastomosis – an anastomosis is a connection or opening between two things that are normally diverging or branching, such as between blood vessels, leaf veins, or streams – involving a division of the small intestine, resulting in a Y-shaped configuration [↩]
Sleeve Gastrectomy (SG) – a surgical weight-loss procedure in which the stomach is reduced to about 15% of its original size, by surgical removal of a large portion of the stomach along the greater curvature. [↩]
Bulimia nervosa is an emotional disorder characterised by a distorted body image and an obsessive desire to lose weight, in which bouts of extreme overeating are followed by fasting or self-induced vomiting or purging. [↩]
Pathophysiology or physiopathology is the disordered physiological processes associated with disease or injury. [↩]
Intra-peritoneal means within or administered through the peritoneum – the thin, transparent membrane that lines the walls of the abdominal (peritoneal) cavity and contains/encloses the abdominal organs such as the stomach and intestines [↩]
systemic administration is a route of administration of medication, nutrition or other substance into the circulatory system so that the entire body is affected. Administration can take place via either, 1. enteral, that is, via the gastrointestinal tract by oral, sublingual, oesophagus, stomach, small/large intestine and rectum, or by 2. parenteral administration, that is via means that bypass the gastrointestinal tract, mainly by intramuscular, subcutaneous, or intravenous injections that bypass skin and mucous membranes [↩]
Morphology is a branch of biology dealing with the study of the form and structure of organisms and their specific structural features. [↩]
radioimmunoassay is a technique for determining antibody levels by introducing an antigen (a toxin or other foreign substance which induces an immune response in the body, especially the production of antibodies) labelled with a radioisotope and measuring the subsequent radioactivity of the antibody component [↩]
PYY (Peptide YY or peptide tyrosine tyrosine) – a peptide that in humans is encoded by the PYY gene. Peptide YY is a short peptide released from cells in the ileum and colon. Soon after eating, and before food reaches the lower small intestine (ileum), PYY is secreted into the blood by cells lining the ileum and colon. [↩]
If you’re not familiar with leptin, it’s certainly familiar with you. Known by various nicknames, such as the ‘satiety hormone’ or ‘fat hormone’, leptin plays a leading role in daily dietary dramas. But, is it more responsible for over-eating (hyperphagia) and obesity than mere lack of will-power?
Blog Contents
What is leptin?
In healthy, non-obese individuals, the hormone leptin controls appetite. After you’ve eaten a meal, this anorexigenic (appetite-suppressing) hormone gets released by adipose tissue (fat cells) and acts on the hypothalamus in the brain to produce a feeling of satiety (fullness) which then suppresses the appetite and (hopefully) stops you from over-eating. It also speeds up your resting metabolism, thereby increasing energy expenditure. 1
This is a pretty sensible mechanism, from an evolutionary point of view, since it would help stop members of our species from getting too fat to be able to run away from sabre-toothed tigers. 2
On the other hand, there were perfectly good reasons why we might have needed to store up as much fat as possible – to get through periods of famine, for instance. 3 This is why there are mechanisms, including the orexigenic (appetite-stimulating) hormone ghrelin (the “hunger hormone“) 4 , which act in the opposite direction from leptin, actively stimulating us to feel hungry. 5
However, evolution wasn’t so good at predicting the appearance of McDonald’s Whoppers or Chocolate Hobnobs. And this is where the problem starts with leptin. If we continue to eat the ‘wrong’ foods, the brain doesn’t realise we’ve actually had enough to eat.
Before looking into a bit more detail about why leptin might not be doing its job properly – evident by the widespread increase in obesity – it’s worth mentioning that other mechanism supposed to help us moderate food intake – namely, stretch receptors in the stomach 6 . If these are supposed to activate as the stomach expands in size, you can see from the above graphic that high-calorie/low-bulk foods will not stretch the stomach as much as low-calorie/high-bulk foods – that is, plant foods which are high in fibre content.
Such foods (mostly processed with high levels of sugar, saturated fat and salt) tend to be high in calories but low in nutrients (such as fibre, vitamins, minerals and phytonutrients). 7 . This is where we come across the differences between toxic hunger and real hunger, as discussed in a previous blog 8 . It’s called “toxic” because it can end up causing us to chronically over-eat and become obese, resulting in all the nasty associated problems like type 2 diabetes, heart disease and various cancers.
Leptin – Animal-Eaters vs Plant-Eaters
So, turning back to leptin, a recent study 9 took a small number of healthy women from three different dietary groups: omnivores, lacto-ovo-vegetarians, and vegans to see if there were any difference in leptin levels between them. What they found was in line with previous studies 101112 , namely: “…people who adopted a vegetarian dietary pattern had lower plasma levels of leptin when compared to the meat consumers.” The mean plasma leptin levels were:
omnivores – 7.45 ng/ml
lacto-ovo-vegetarians – 3.87 ng/ml
vegans – 2.89 ng/ml
Leptin & Obesity
It’s well-established that meat-eaters are more likely than plant-eaters to become obese1314 . So, does this mean that meat-eaters don’t have enough leptin to inform their brains that they have eaten enough, and that plant-eaters have too much leptin? Oddly enough, quite the reverse.
Leptin Insensitivity/Resistance
What’s actually happening is that the abundance of swollen fat cells produce so much leptin that the hypothalamus starts to become insensitive and eventually resistant to leptin’s action. Thus, the brain keeps telling the obese individual “You’re still hungry!“. Eating plant-based diets – ideally WFPB diets, since vegan diets can still lead to obesity if they contain loads of junk food 15 – does not result in such fat storage in the body and, hence, leptin continues to do its job without the body getting “fed up of it”…
You’ve probably already drawn a parallel here with leptin resistance/insensitivity – namely, to type 2 diabetes. By definition, T2D is a condition which transitions through a stage where the pancreas still pumps plenty of insulin into the bloodstream, but cells become resistant/insensitive to it 16 .
It’s similar to how taste buds become insensitive to salt and sugar, how one can develop tolerance for cigarettes or alcohol, even though the body is silently screaming.
Do I Need To Increase Leptin levels?
Perhaps the more appropriate question should be “How do I make my body more sensitive to the already high levels of leptin in my body?”
The simplest and healthiest way is likely to be through changing to a plant-based diet. Not only is this likely to clear up any existing problem with leptin resistance, it will also help to reverse a huge range of diseases – including obesity 17 , type 2 diabetes 18 , cardiovascular disease 19 , and even many cancers 20 .
Final thoughts
The above brief analysis has suggested that, A. leptin works best within non-obese bodies and, B. that non-obese bodies are more likely to be inhabited by plant-eaters than by meat-eaters.
We also know that plant-eaters are less likely than omnivores to suffer from metabolic syndrome – a complex of conditions in which triglycerides, total cholesterol, low-density lipoprotein (LDL), blood glucose, blood pressure, waist circumference, and body mass index (BMI) are all increased to seriously unhealthy levels21 .
It’s The Fat!
And much of the problem is simply to do with the amount of fat within the body – not that we grow more fat cells, since we actually retain a reasonably constant number of fat cells throughout adult life 22 , rather the fat cells we have can grow and grow until they’re so stuffed full that they leach fat back into the bloodstream without us even needing to consume any dietary fat – a process known as “reintoxication” 23 Yuk!
So What About Will-Power?
It’s so easy to think that overweight/obese individuals lack sufficient will-power. However, it may be more likely that they are simply acting in accordance with what their brain is telling them or, rather, what their brain is failing to tell them.
How Do I Know If I’m Leptin Resistant?
It may sound too simple, but – just look in the mirror or see if you can grab a handful of fat around the middle of your body. Basically, there’s a really strong chance that leptin is not doing its job inside you if you are overweight.
How Do I Reverse Leptin Resistance?
I keep hammering away at this…but, all the evidence strongly suggests that the healthiest, most natural and sustainable diet for weight loss, general disease-resistance and healthy longevity is a wholefood plant-based diet. 2425 . It’s also probably the healthiest for the rest of life on Earth, too 26 .
How about having a go at the short quiz below?
[qsm quiz=18]
References
Waugh, Anne; Grant, Allison. Ross & Wilson Anatomy and Physiology in Health and Illness E-Book (p. 284). Elsevier Health Sciences. Kindle Edition. [↩]
Ghrelin is the primary hunger hormone. It’s released from your stomach (with smaller amounts being released by the small intestine, pancreas and brain) into the blood and to the brain to stimulate hunger to alert you that you’re hungry. It has many functions throughout your body besides hunger. It also functions within the pleasure/reward centre of the brain, and plays a role in memory formation, immune function, and even sleep. [↩]
If you count yourself among the one in three vegans choosing a plant-based diet for health reasons1 , then think again before following the thronging crowds to pig out (if that’s not speciesist) on the growing range of vegan fast foods – particularly yummy burgers that try so hard to imitate those traditionally made from meat.
Blog Contents
The article
A reader sent me an article, entitled “Vegan burgers can contain more saturated fat than TWO McDonald’s Big Macs” 2 , which basically expanded on what’s clear from the article’s title.
Saturated fat – what’s the problem?
Consuming even moderate quantities of saturated fat has been proven 345 to be a really dumb option – if, that is, you want to be healthy. Naturally, if you don’t care about your health and the length of your useful life, then eating foods with saturated fat – especially if they’re also accompanied by lots of sugar, oil, salt and cholesterol – will certainly titillate your taste buds, while, of course, simultaneously totalling your ticker.
And it’s not just your heart that cringes when it sees those burgers or fatty patties approaching the hallowed doors of your intestinal tract. The following are just some of the conditions with strong links to saturated fat consumption 6 :
Oh, and I nearly forgot, also MS (Multiple Sclerosis), covered in detail in a previous blog 7 .
Surely vegan burgers can’t be that bad…they’re vegan!
This is the list of burgers mentioned in the article:
You’ll notice Marstons’ Moving Mountain’s B12 and Aldi’s The Meat Free Butcher: Juicy Quarter Pounder vegan burgers each contain more saturated fat than a McDonald’s Big Mac, and the vegan All Bar One Beyond Burger has more than a standard McDonald’s hamburger. Only Iceland’s vegan No Bull Burger drops below the saturated fat content of McDonald’s meaty offerings.
What’s the recommended daily allowance of saturated fat?
The answer to this depends on whether you want to eat the recommended amount for normal people who end up having all the normal diseases. If so, then the UK government health recommendations 8 are that the average man aged 19-64 years should eat no more than 30 g of saturated fat a day, while the average woman aged 19-64 years should eat no more than 20 g of saturated fat a day. Less for people younger or older than this. Meanwhile, the US FDA recommendations9 are that less than 20 g per day should be eaten, based on a 2,000 calorie diet – higher or lower depending on calorie requirements.
However, if you want the hard truth about tolerable limits of saturated fat (or trans fats or cholesterol) the answer is that anything above zero is not tolerable. “The Institute of Medicine did not set upper limits for trans fat, saturated fat, and cholesterol because any intake level above zero increased bad cholesterol (LDL cholesterol).” 510
What’s the saturated fat in vegan burgers?
Usually it’s coconut oil – one of the few plant-derived foods that is not recommended at all as part of a WFPB diet. A previous blog 11 , entitled “Coconut Oil is ‘Pure Poison’ says Harvard Professor” dealt with this Frankenfood12 in more detail.
Pause for a giggle
At the start of this Mirror online article about the dangers of processed vegan foods, it was rather ironic that the video-advert included was for another super-unhealthy ultra-processed food:
They just can’t stop themselves, can they?
Final thoughts
It’s no surprise that these ultra-processed 1314 vegan burgers, and similar vegan fast foods, are modified in order to appeal to our vulnerable taste buds, in just the way that similar meat-based products are; but the fleeting buzz from all that fatty nonsense is always closely followed by a nasty sting. And whether you consciously feel it or not, the cells, tissues and organs within your body certainly do. You just have to look at some of the mass of research on dietary saturated fats, using brachial artery flow‐mediated dilation tests1516171819202122 , to see how much immediate damage is caused by consuming these foods.
Since coconut oil is 100% fat with 87% being saturated fat, my best advice to you is, if you come across a product that contains it, avoid it like the plague.
It gets repeated time and time again on this website, but the only way you can be absolutely certain you’re avoiding all these dietary pitfalls and food industry tricks is to eat the optimal diet for human health and longevity: a non-SOS WFPB diet.
A major 2018 prospective study 1 , involving 104,980 French participants, shows a shocking link between ultra-processed foods and cancer. And don’t think that this term ‘ultra-processed’ refers to foods that most of us are unlikely to eat – unless you eat an exclusively non-SOS WFPB diet, most people in our societies are most likely to be eating these foods on a regular basis.
Blog Contents
At the risk of repeating myself…
Whilst the press is treating this research as having just been released2 , a previous blog3 looked at this research when it was first published in February 2018 (maybe it takes this length of time for the mainstream media to catch up with such research findings). In any case, because the information is so important, it seems worthwhile reiterating some points, as well as processing some food definitions .
The Study
The BMJ study, entitled “Consumption of ultra-processed foods and cancer risk: results from NutriNet-Santé prospective cohort study“, looked for associations between ultra-processed food intake and risk of overall, breast, prostate, and colorectal cancer. To do this, they followed a large number of individuals for over 8 years, getting a wide range of data from them and analysing the results to see if there was a convincing link between consumption of so-called ‘ultra-processed foods’ and various forms of cancer.
Study Results
And, yes, they did. They concluded:
“In this large prospective study, a 10% increase in the proportion of ultra-processed foods in the diet was associated with a significant increase of greater than 10% in risks of overall and breast cancer.”
Pretty clear confirmation of a relationship although, of course, in any observational study, no matter how long and far-reaching, there’s always a question of whether a causal relationship exists between the two variables.
Irrespective of Dietary Habits
The relationship between 10% increase in ultra-processed food consumption and over 10% increased risk of developing various forms of cancer did not vary with diet. This means that, regardless of whether you’re a vegan, vegetarian, omnivore, or have a higher or lower ratio of particular macronutrients (carbs, fat or protein) in your diet, the risk remained statistically the same: anyone, no matter how healthy your diet, eating these ultra-processed foods appears to have their risk of cancer increased by the same percentage.
The 4 Definitions of Processed
In the study, they define 4 groups of foods, as outlined by the NOVA Group 4 .
a. Unprocessed or b. minimally-processed foods
Processed culinary ingredients
Processed foods
Ultra-processed food and drink products
I’m going to explain the above 4 classifications in a fair bit of detail. I think this important since most of us are going to get confused by what differences exist between these groups. Indeed, most of only use two terms, “unprocessed” and “processed”, and even this is mostly done without being absolutely certain what we’re really talking about.
Group 1. Unprocessed or minimally processed foods
a. Unprocessed(or natural) foods are edible parts of plants (seeds, fruits, leaves, stems, roots) or of animals (muscle, offal, eggs, milk), and also fungi, algae and water, after separation from nature.
b. Minimally processed foods are natural foods altered by processes such as:
None of these processes adds substances such as salt, sugar, oils or fats to the original food.
The main purpose of the processes used in the production of group 1a. foods is to extend the life of unprocessed foods, allowing their storage for longer use, such as chilling, freezing, drying, and pasteurising.
Other purposes include facilitating or diversifying food preparation, such as:
removal of inedible parts
fractioning vegetables
crushing or grinding seeds
roasting coffee beans or tea leaves
fermentation of milk to make yoghurt
Foods included in Group 1:
fresh, squeezed, chilled, frozen, or dried fruits and leafy and root vegetables
grains such as brown, parboiled or white rice, corn cob or kernel, wheat berry or grain
legumes such as beans of all types, lentils, chickpeas
starchy roots and tubers such as potatoes and cassava, in bulk or packaged
fungi such as fresh or dried mushrooms
meat, poultry, fish and seafood, whole or in the form of steaks, fillets and other cuts, or chilled or frozen
eggs
milk, pasteurised or powdered
fresh or pasteurised fruit or vegetable juices without added sugar, sweeteners or flavours
grits, flakes or flour made from corn, wheat, oats, or cassava
pasta, couscous and polenta made with flours, flakes or grits and water
tree and ground nuts and other oil seeds without added salt or sugar
spices such as pepper, cloves and cinnamon
herbs such as thyme and mint, fresh or dried
plain yoghurt with no added sugar or artificial sweeteners added
tea, coffee, drinking water
Group 1 also includes foods made up from two or more items in this group:
dried mixed fruits
granola made from cereals, nuts and dried fruits with no added sugar, honey or oil
foods with vitamins and minerals added generally to replace nutrients lost during processing, such as wheat or corn flour fortified with iron or folic acid
Group 1 items may infrequently contain additives used to preserve the properties of the original food:
vacuum-packed vegetables with added anti-oxidants
ultra-pasteurised milk with added stabilisers.
Group 2 – Processed culinary ingredients
These are substances obtained directly from group 1foodsor from nature by processes such as:
pressing
refining
grinding
milling
spray drying
Purpose of processing – to produce products that can be used in both home and restaurant kitchens to prepare, season and cook group 1 foods and to make with them varied and enjoyable hand-made dishes, soups and broths, breads, preserves, salads, drinks, desserts and other culinary preparations.
Group 2 items are rarely consumed in the absence of group 1 foods, for instance:
salt mined or from seawater
sugar and molasses obtained from cane or beet
honey extracted from combs
syrup from maple trees
vegetable oils crushed from olives or seeds
butter and lard obtained from milk and pork
starches extracted from corn and other plants
Products consisting of two group 2 items remain in this group, such as:
salted butter
group 2 items with added vitamins or minerals (e.g. iodised salt)
vinegar made by acetic fermentation of wine
some alcoholic drinks (see group 4)
Group 2 items may contain additives used to preserve the product’s original properties, such as:
vinegar with added preservatives that prevent microorganism proliferation
Group 3. – Processed foods
These are relatively simple products made by adding sugar, oil, salt or other group 2 substances to group 1 foods. Most processed foods have two or three ingredients.
Processes include various preservation or cooking methods, and, in the case of breads and cheese, non-alcoholic fermentation.
Main purpose of processed food manufacture is to increase durability of group 1 foods, or to modify or enhance their sensory qualities.
Typical examples of group 3 processed foods include:
canned or bottled vegetables
canned or bottled fruits and legumes
salted or sugared nuts and seeds
salted, cured, or smoked meats [including fish]
canned fish
fruits in syrup
cheeses
unpackaged freshly-made breads
Processed foods may contain additives used to preserve their original properties or to resist microbial contamination. For instance:
fruits in syrup with added anti-oxidants
dried salted meats with added preservatives
alcoholic drinks produced by fermentation of group 1 foods (such as beer, cider and wine)
Group 4. – Ultra-processed food and drink products
These are industrial formulations typically with five or more and usually many ingredients, including those also used in group 3 processed foods, such as:
sugar
oils
fats
salt
anti-oxidants
stabilisers
preservatives
Ingredients only found in group 4 ultra-processed products include:
substances not commonly used in culinary preparations
additives whose purpose is to imitate sensory qualities of group 1 foods
additives whose purpose is to imitate culinary preparations of group 1 foods
additives used to disguise undesirable sensory qualities of the final product
Group 1 foods are a small proportion of or are even absent from group 4 ultra-processed products.
Substances only found in ultra-processed products include:
some directly extracted from foods, for instance:
casein
lactose
whey
gluten
some derived from further processing of food constituents, for instance:
Several industrial processes with no domestic equivalents are used in the manufacture of group 4 ultra-processed products, such as extrusion15 , moulding and pre-processing for frying.
The main purpose of industrial ultra-processing is to create products that are ready to eat, to drink or to heat. Unfortunately, these will probably replace both unprocessed or minimally processed foods in the diet – the latter being naturally ready to consume, such as fruits and nuts, milk and water, and freshly prepared drinks, dishes, desserts and meals.
Common attributes of group 4 ultra-processed products are:
hyper-palatability
sophisticated and attractive packaging
multi-media and other aggressive marketing to children and adolescents
health claims
high profitability
branding/ownership by transnational corporations
Examples of typical group 4 ultra-processed products include:
carbonated drinks
sweet or savoury packaged snacks [including crisps – potato chips in the US]
ice-cream
chocolate
candies (confectionery)
mass-produced packaged breads and buns
margarines and spreads
cookies (biscuits)
pastries
cakes and cake mixes
breakfast ‘cereals’
‘cereal’ and ‘energy’ bars
‘energy’ drinks
milk drinks
‘fruit’ yogurts
‘fruit’ drinks
cocoa drinks
meat and chicken extracts
‘instant’ sauces
infant formulas
follow-on milks
other baby products
‘health’ and ‘slimming’ products, such as:
powdered meal substitutes
‘fortified’ meal substitutes
many ready to heat products, including:
pre-prepared pies
pasta dishes
pizza dishes
poultry ‘nuggets’
fish ‘nuggets’ or ‘sticks’
sausages
burgers
hot dogs
other reconstituted meat products
powdered and packaged ‘instant’ soups
‘instant’ noodles
powdered and ‘instant’ desserts
Group 4 foods also include any products made solely of group 1 or group 3 foods which also contain cosmetic or sensory intensifying additives, such as:
plain yoghurt with added artificial sweeteners
breads with added emulsifiers
Group 4 also includes any alcoholic drinks which are identified as foods which are produced by fermentation of group 1 foods followed by distillation of the resulting alcohol, such as:
whisky
gin
rum
vodka
Everything but group 4’s okay, then?
Short answer? No.
Adding single additives like salt16 , sugar17 , and oils18 have detrimental effects on health. All animal foods are associated with serious health issues 19 , compared with plant foods 20 . Cured/smoked fish, in particular, though it’s in group 3, has been shown to be carcinogenic 21 .
It’s also worth noting that this is a survey from the country historically known to be the centre of culinary excellence – noted for its supposedly health Mediterranean diet 18 . It would be no surprise, then, that populations in other Western countries – particularly the UK and USA22 – have considerably more consumption of ultra-processed foods.
All clear now?
If you’ve got all the food types, food combinations and preparation methods nice and sorted in your head, then you’re cleverer than most of us. Whilst some elements have been made clear by this research, there remains some lack of clarity about which items out of groups 1 to 3 might still cause adverse effects.
Perhaps, the only sure way to know that the foods you are eating offer optimal protection against developing cancer is to eat a non-SOS WFPB diet. Foods on the plate that look remarkably similar to how they looked when they were first harvested.
Podcast by the authors
You may be interested in listing to a short podcast 23 , where two of the authors of the above study are interviewed by a representative from the BMJ (British Medical Journal):
Final thoughts
It would surprise me greatly if many people reading this could say with hand on heart that they never eat any of the above group 4 foods. They have become such a mainstay of our modern Western diets that they go largely unnoticed and accepted without question.
Are the scientists helping?
Have you ever heard anyone talking about ‘ultra-processed’ foods before? Of course not – we conventionally refer to group 4 foods as simply ‘processed foods’.
Whether the likes of McDonald’s Egg McMuffin or Walker’s Prawn-Flavoured Crisps will ever be referred to as ‘ultra-processed’ foods by the general population is, I think, unlikely. So, once again, there’ll be an unfortunate disconnect between the technical terms used in scientific reports and the terminology used ‘on the street’.
However, the study makes one thing certain: If you want to maintain optimal health and longevity, you’re not going to get it by eating the processed foods that most people eat, most days.
With a greater than 10% increase of an early (probably painful and humiliating) death from every 10% increase in the percentage of processed (group 4) foods we can’t resist stuffing into our mouths – what’s the difference between eating this junk or smoking a few cigarettes a day?
Finally, you may like to have a go at the quiz below.
“Fractioning” foods or, simply, “fractionation” is a separation process in which a certain quantity of a mixture (gas, solid, liquid, enzymes, suspension, or isotope) is divided during a phase transition, into a number of smaller quantities in which the composition varies according to a gradient. [↩]
An anti-humectant (or anti-humidity) product is a moisture blocker which aims to resist potential moisture intrusion. [↩]
Hydrogenated oils are oils treated with hydrogen. It is a chemical reaction between molecular hydrogen and another compound or element, usually in the presence of a catalyst such as nickel, palladium or platinum. The process is commonly employed to reduce or saturate organic compounds.
interesterified oils ((Interesterified oils or fat is a type of oil where the fatty acids have been moved from one triglyceride molecule to another. This is generally done to modify the melting point, slow rancidification and create an oil more suitable for deep frying or making margarine with good taste and low saturated fat content. [↩]
Hydrolysed protein is a protein that has been at least partially hydrolysed or broken down into its component amino acids. While many means of achieving this exist, two of the most common methods are prolonged boiling in a strong acid or strong base (alkaline), or using an enzyme such as pancreatic protease to simulate the naturally occurring hydrolytic process, where hydrogen and oxygen molecules in water are separated using electricity. [↩]
Soy protein isolate is produced through a process called hexane extraction. The fats are separated from the soybean in a hexane bath. Hexane is a gasoline byproduct and the USDA classifies it as a neurotoxin which they do not allow to be used in food defined as organic. Once the fats are removed from the soybean, it’s then soaked in an ethanol or an acidic bath to remove carbohydrates and any lingering flavour. [↩]
Maltodextrin is a polysaccharide that is used as a food additive. It is produced from starch by partial hydrolysis and is usually found as a white hygroscopic spray-dried powder. Maltodextrin is easily digestible, being absorbed as rapidly as glucose and might be either moderately sweet or almost flavourless. [↩]
Inverted sugar (also called inverted sugar syrup) is a mixture of two simple sugars – glucose and fructose. It’s made by heating sucrose with water. Sweeter than table sugar, the foods containing it can retain moisture and, thus, crystallise less easily. Bakers, who call it ‘invert syrup’, may use it more than other sweeteners. [↩]
A sequestrant is a food additive which improves the quality and stability of foods. A sequestrant forms chelate complexes with polyvalent metal ions, especially copper, iron and nickel, which can prevent the oxidation of the fats in the food. Sequestrants are a type of preservative. [↩]
Extrusion is is a process by which a set of mixed ingredients are forced through an opening in a perforated plate or die with a design specific to the food, and is then cut to a specified size by blades. [↩]
Surely dates taste far too nice to be good for us! Isn’t there a catch? Well, it appears research is pretty clear about whether or not eating seven dates a day is a healthy option. We’ll look specifically at whether such a sweet addition to the daily diet helps to protect against colon cancer. In addition, some other surprising potential benefits will also come under scrutiny.
Blog Contents
Antioxidant content of sweeteners
Compared with other sweeteners, date sugar (a powder made simply from powdered dried dates) has the most antioxidants, as shown in the following chart 1 :
Other health claims for dates
One study 2 makes pretty wide claims about the benefits of dates for a whole range of diseases – although the research was based largely on experiments with rats:
Although there needs to be more research regarding several of the above claims before drawing final conclusions, there are at least two of the benefits mentioned for which there’s support from some compelling studies – namely, aiding relaxation during labour and delivery34567 and possessing an anti-tumour effect . Dr Greger has a couple of videos on the former (i.e. dates and pregnancy) 89 , if you’re interested. However, our main focus here is on the anti-tumour (anti-cancer) effects, particularly with regard to the colon.
Dates & the colon
Although this sounds like some 70’s Punk Band, dates seem to be seriously beneficial for the colon.
In several earlier blogs 10111213 , we looked at health issues related to the bacteria in our guts (variously referred to as ‘gut flora‘, ‘gut microbiome‘ or ‘gut microbiota‘ – technically, ‘microbiota’ refers to the microbes found in a specific environment, while ‘microbiome’ is the whole collection of microbial genomes in that environment. In any case, the billions of bacteria living inside us seem to have astonishingly diverse and far-reaching influences on every aspect of human health – from psoriasis and MS to depression and fibromyalgia.
Central to the ability of the microbiota to do their best work for us, is the type of foods we consume – with prebiotics, such as fibre and polyphenols (a type of antioxidant phytonutrient), being really important to get the best out of these little chaps (and chapesses?). And, weirdly inappropriate gender allusion aside, it just so happens that dates contain lots of these prebiotics.
Dates in vitro
Research 14 has shown the ability of dates (at least, in these in vitro tests), not only to increase the amount of ‘good’ bacteria, but also to kill off colon cancer cells. The researchers concluded: “…consumption of date fruits may enhance colon health by increasing beneficial bacterial growth and inhibiting the proliferation of colon cancer cells. This is an early suggestion that date intake by humans may aid in the maintenance of bowel health and even the reduction of colorectal cancer development.”
Dates in vivo
Of course, the latter were in vitro and not in vivo tests – that is, in a petri dish rather than in a dishy Peter (or Polly, for that matter). However, a subsequent randomised, controlled, cross-over, intervention study 15 , which looked for similar effects in actual human beings, found that consumption of seven dates for three weeks:
1. Significantly increases bowel movements and stool frequency
The additional fibre will play a big part here. Having regular (and easy!) bowel movements is, of course, a strong sign of good bowel health – helping to prevent constipation, diverticulosis (which can develop into diverticulitis), hiatal hernias, heartburn, GERD, etc. When eating a high fibre diet, two or three healthy bowel movements each day are quite normal. With enough fibre in the stool, you should be able to sit in any position and have a comfortable bowel movement 16 .
In terms of long-term ‘uncomfortable’ or infrequent bowel movements and the development of colon cancer, one study concludes: “Constipation was associated with a moderately increased risk of colorectal cancer.” 17 , while another study concludes: “Patients with chronic constipation are associated with significantly higher prevalence and incidence of colorectal cancer and benign colorectal neoplasm than matched chronic constipation‐free patients. These risks increase with the severity of chronic constipation.” 18 .
Now, there is some debate about whether there’s a causal link between chronic constipation and colon cancer (also referred to as colorectal cancer or CRC, which covers the rectum as well as the colon). But why take the chance?
So what? Isn’t ammonia an alkaline? And previous blogs 1920 have encouraged us to eat a morealkaline diet, even suggesting we use a litmus paper test to ensure we produce alkaline urine. So why wouldn’t it be a good thing to have alkaline poo?
Well, in overly simplistic terms, alkaline urine is good and alkaline poo is bad.
Back in 1981, a study 21 stated: “Considerable evidence suggests that the carcinogens or co-carcinogens responsible for the development of colorectal cancer are either bacterially degraded bile acids or cholesterol. It is proposed that a high colonic pHpromotes co-carcinogen formation from these substances…“
This potentially carcinogenic process is inhibited once the pH of stools drops below a pH of 6.5 – around the alkalinity of milk. The same study largely blames alkaline poo on a lack of vegetables in the diet, and recommends dietary changes that increase fibre content (i.e. eat more veggies), which gut bacteria will then break down to short-chain fatty acids (SCFA’s) and thereby help to neutralise the problem.
Following this, a 1982 population study 22 confirmed the above hypothesis, showing that those with a faecal pH of 8 or above (around the pH of eggs, by the way) were at particular risk of developing colon cancer.
A 2013 study 23 found that African Americans were 50-times more at risk of colon cancer then Native Africans, concluding: “Our results support the hypothesis that colon cancer risk is influenced by the balance between microbial production of health-promoting metabolites such as butyrate and potentially carcinogenic metabolites such as secondary bile acids.“
The importance of dietary fibre for the production of butyrate (and other SCFA’s such as propionate and acetate) was shown in previous blogs 2425 , as was the importance of the metabolism of bile acids26 in relation to alcohol-consumption.
The researchers continued: “In summary, our study supports the hypothesis that colon cancer risk is determined by the interaction between diet and gut microbiota 2728 and that the higher risk in African Americans could be attributed to their chronically lower consumption of [soluble] fiber and resistant starch [insoluble fibre] and their higher consumption of dietary fat.” Furthermore, “The higher consumption of animal protein is one possible explanation for higher stool pH values in subjects on an omnivorous diet, as proteolytic putrefaction bacteria are able to increase stool pH by producing alkaline metabolites [such as ammonia].” 29
In one of his videos, “Testing Your Diet with Pee & Purple Cabbage” 30 , Dr Greger provides a clear explanation of why it is that we should be looking for purple poo and blue pee, when using his ‘red cabbage water down the loo’ technique!
3. Significant reduction in faecal genotoxicity
What this means is that eating those seven dates for just three weeks resulted in significantly less DNA-damage. This is really important, being that the inside protective walls of the colon are made up of DNA.
A 2015 study 31 looked in more detail at the the relationship between date-consumption and cancers. They did in vitro testing of whether or not dates (and they used a rather wide-range of different varieties) were able to kill off various cancer cells from common cancers, including:
stomach cancer
prostate cancers
colon cancer
breast cancer, and
lung cancer
They concluded: “…extracts from all 29 varieties of date fruits showed that it contained components than can act as reducing agents and free radical scavengers in cellular reactions in vivo…” It’s a well-accepted fact that free radicals are known to cause DNA-damage 32 , and that DNA-damage, in turn, is the major cause of cancer33 .
“…Similarly, the inhibition of COX enzymes [enzymes responsible for prostanoid-formation] indicated that the extracts contain compounds that can inhibit the production of inflammation causing hormones such as prostaglandins and thromboxanes by preventing the formation of prostaglandin endoperoxide which then leads to the production of inflammatory intermediates…” We’ve seen before 34 how inflammation is responsible for considerable damage within the body – often leading to cancer-formation, and how plant-based diets are anti-inflammatory, while animal-based diets are pro-inflammatory.
“…These results further support the health-benefits of date fruits over and above its nutritional value. The bioassay results also suggest that most varieties of date fruits studied provide similar levels of health benefits.“
This may once again suggests just how interlinked everything is within our bodies, and provides additional support for a wholistic (that deals with the whole body) rather than a reductionist (one that deals with each cell, tissue, organ, or disease as relatively separate and unrelated entities) approach to human nutrition and general health. 35 We’re still relatively ignorant, not only about the true complexity and inter-relatedness of the nutrients we consume, but even about the sum total of nutrients that have not even been identified or named yet.
Naturally, the latter is an in vitro study, and more in vivo research is needed to establish any causal relationship between date-consumption and cancer-prevention/treatment. What was especially interesting in the latter results was that the positive effects were not just on the cancer cells normally coming into direct physical contact with the contents of our gastrointestinal tracts (that is, stomach and colon), but that cancer cells from other organs (prostate, breast and lung) were also killed by the date extract.
Final thoughts
In terms of constipation-avoidance, dates will, of course, only play a small part in alleviating or preventing this unpleasant and potentially dangerous condition. Eating a WFPB diet – including the seven daily dates – will ensure that you’re doing the best for the smooth-running within the plumbing “down there”, as my mother used to say…
Avoiding high levels of saturated fat and animal protein, while filling up on the fibre-rich plant foods, appears to be the way to ensure that what comes out of our bottoms falls on the right side of the pH scale. This is borne out by research 3637 on plant-based diets and how their gut microbiome was populated by more health-beneficial bacteria species, such as Bifidobacterium and Lactobacillus, when compared with the typical omnivore Western diets. And such ‘good’ bacteria are responsible for releasing organic products such as lactic acid and acetic acid, which decreasepH value. So, once again, it’s the plant foods, including dates, of course, that keep it all above board down below.
If just seven dates a day for three weeks can reduce both free radicals and inflammation, what’s to be lost in making them a daily staple? I simply chop up seven dates and add them to my daily fruity-muesli breakfast – making sure there are no stones accidentally left lurking within, of course.
Finally, you may be interested in having a go at the little quiz below, covering aspects of this blog.
Further to recent blogs on breakfasts 1 and the ‘bliss point’ in processed foods 2 , I thought it would be interesting to take a more detailed look inside the body, just to see what actually happens when a highly processed sugary product, specifically Kellogg’s Frosties, meets the inside of a human body – touching on associated issues, ranging from insulin resistance and cellular respiration to diabesity and non-alcoholic fatty liver disease.
Blog Contents
Grrreat for whom?
It’s quite true that such breakfast cereals are great for the manufacturer’s profit and loss account, but what’s their true cost in terms of human health?
In order to understand what happens to those sweet, crunchy morsels once they get into our bodies, we’ll need to delve into a bit of nutritional science. So here goes…
Frosties – ingredients & nutritional information
As you will see from the footnote below 3 , a 100 g of Frosties contains 87 g processed carbohydrates, 37 g of which is pure sugar (specifically, sucrose – a disaccharide consisting of one glucose and one fructose molecule). The carbohydrates are processed to remove nearly three quarters of the fibre contained in the original whole corn (also called maize) – 2 g/100 from 7-8 g/100 g in whole corn. This gives Frosties a glycaemic index (GI) of 51 compared to 100 for pure glucose 4 . To its credit, Frosties is at least fortified with several vitamins and doesn’t contain any palm oil.
From mouth to bloodstream
As soon as Frosties enter the mouth, the carbohydrate-digesting enzyme amylase produced in saliva starts to break down the sucrose into its two monosaccharides, glucose and fructose, and the lump of food in the mouth is then referred to as a ‘bolus’.
From the mouth, the bolus passes to the stomach, during which time it magically changes its name to ‘chyme’ – a pulpy acidic fluid consisting of gastric juices and partly-digested food.
From the stomach, the chyme passes into the first part of the small intestine, the duodenum.
A signal then passes to the pancreas for it to release pancreatic amylase along a duct and into the duodenum.
At this point, a number of enzymes have pretty much completed the digestion of the sugars and any starches, producing the end product of the monosaccharide, glucose.
The resulting glucose within the mixed contents of the intestine (the ‘lumen’) then passes through the wonderfully complex epithelial membrane and into the bloodstream through an absorption process called ‘active transport’.
Here comes the insulin – hopefully…
Once the glucose levels rise in the bloodstream, the beta cells of the islets of Langerhans within the pancreas detect this increase and release the hormone, insulin – in healthy individuals, that is.
The situation is different for those with type 1 diabetes (T1D), where the pancreas does not produce insulin (or only very small quantities).
For those with type 2 diabetes (T2D), the situation is not the same, since plenty of insulin may be released from the pancreas but, for reasons covered below, fails to do its job properly.
If blood glucose levels are too low, another hormone called glucagon is released into the bloodstream, this time from the alpha cells in the islets of Langerhans within the pancreas.
Glucagon’s function is to instruct the release of some glucose which has been stored as glycogen in the liver and muscle cells (a process called glycogenolysis).
This is just one of the wonderful examples of homeostasis – a continual balancing act occurring within our bodies every second of every day. Put simply:
when blood glucose levels rise above a certain level, the pancreas produces more insulin
when blood glucose levels fall below a certain level, insulin production stops and glucagon production starts
From blood to cell
In our scenario, the sugar in the Frosties has been converted into glucose and has ended up in the bloodstream. Insulin’s main job now is to get that glucose into the body’s cells. If it does so successfully – and this is the big IF when it comes to those with T2D – the glucose is oxidised in the cells (that is, the glucose combines chemically with oxygen) and becomes a source of energy. This intracellular energy-production process is known as ‘cellular respiration’.
Cellular respiration (also known as internal respiration) is a complex process, involving three metabolic pathways: glycolysis, the citric acid (Krebs) cycle, and oxidative phosphorylation; but the important result is that the glucose from our Frosties is converted into energy. This energy is in the form of ATP (adenosine triphosphate), known as the “molecular (or energy) currency” of intracellular energy transfer. This only takes place within cells, mostly within the mitochondria (the ‘energy factories’) but also, to a lesser degree, within the cytoplasm of the cell. The product is the energy our bodies require for every function.
If there’s any excess glucose which is not required immediately, it will get stored as glycogen in the liver or skeletal muscles for future use (a process rather confusingly called glycogenesis – the reverse process to glycogenolysis).
If you’re interested in a little more detail on the process of carbohydrate metabolism not covered above, see the note 5 below.
Now comes the spike
If glycogen reserves in the liver are saturated, the excess glucose gets converted into fat for long-term storage in the adipose (fat) tissues – beneath the skin (subcutaneous fat), around internal organs (visceral fat) and in bone marrow (yellow bone marrow).
Because Frosties contain highly refined carbs, rather than the complex starchy carbs found in whole plants, the glucose is released very rapidly. Basically, the more processed the carbs, the quicker they end up as glucose in the bloodstream. Thus, the Frosties are likely to cause what is called an initial ‘insulin spike‘.
In the long term:
insulin spikes can cause serious and irreversible damage to organs, nerves, and blood vessels
there’s likely to be an excess of glucose produced as a result of eating such foods as Frosties – unless you’re running fast on a treadmill when you’re eating! This means that regular consumption may lead to increased body fat and all the health problems associated with that
In the short term:
the sudden hit of these simple carbs (the ‘sugar rush‘) is likely to upset the delicate balance in the blood sugar level and is known to cause some fluctuations in energy levels and mood over the following hours – which could leave the person irritable and tired as the ‘sugar crash‘ arrives and glucose levels settle back to normal
it’s also likely that the person will feel hungry again very soon, since they didn’t get enough of the other nutrients to sustain energy, like protein and fibre
while eating the Frosties, the person’s brain would have responded to the sugar by creating a surge of the “feel-good” brain chemicals dopamine and serotonin. This also happens with certain drugs, such as cocaine. In a similar way to a drug, the body craves more after the initial high. This is one of the reasons that it is very much easier to overeat simple carbs, while complex starchy carbs don’t have the same effect
When the spikes have burst the insulin bubble
Prediabetes6 – arguably a disease in itself – usually takes a number of years to develop into full-blown T2D, where muscle and other cells stop responding to insulin. Known as insulin resistance, this condition causes blood sugar and insulin levels to stay high long after eating. The excessive demands made on the insulin-making cells can eventually wear them out so much that insulin production can eventually cease. 7
Insulin resistance & diabetes
Before pinning down what insulin resistance is, we probably need to be clear on just what diabetes is.
As far back as a 1927 study8 , a clear link between diabetes and fat consumption was demonstrated. In this study, young, healthy people were split into two groups: half were put on a fat-rich diet, and the other half were put on a carb-rich diet. Within just two days, glucose intolerance rose alarmingly in the fat-rich group, with twice as much blood sugar as the carb-rich group. The same principle revealed in this study has been duplicated and confirmed ever since, namely:
as fat in the diet rises, blood sugar spikes rise
Why is this? As it happens, it took around seven decades before the answer could be provided and, thus, form the basis of the current understanding of the cause of T2D. In basic terms, fat in the cells blocks insulin from being able to usher glucose into the cells to be used as energy. As a result of this, the sugar stays in the bloodstream, eventually filling available organs and muscle cells with fat, and reaping havoc on the body as a whole.
Every vampire needs an invitation
“Prepare ye the way for the Lord”!
I think it was Dr Greger who drew the comparison between blood sugar (glucose) and vampires. Just as a vampire requires an invitation before entering private homes, glucose needs an invitation before it can enter our cells. Within our bodies, that invitation comes in the form of insulin.
When a cell requires additional energy, it binds to one of the insulin molecules passing by in the bloodstream and that molecule binds to a specific insulin receptor on the surface of the cell membrane. Once there, the insulin acts like a key, opening up a ‘gap’ in the cell membrane – through the release of a number of enzymes – so that glucose, also circulating in the bloodstream, can enter the cell. It’s important to understand that there’s no other way that glucose can enter the cell than through this insulin receptor.
Glucose (C6H12O6) is a large molecule with 6 carbon atoms. As such. it’s too big to get into the cell through simple diffusion. This is why it needs its own John the Baptist (insulin) to ‘prepare the way for the load‘. The term used for this is ‘facilitated diffusion‘ (also known as ‘facilitated transport’) and it happens down a concentration gradient – that is, it will only happen when there’s more glucose outside the particular cell than there is inside it. If the cell has sufficient glucose inside already, it will close up the insulin receptor and no more glucose will get inside, until more is required.
This form of glucose transport within our muscles is responsible for clearing around 85% of the glucose from our blood.
By the way, all of this is something a simplification of the whole process, of course. In actual fact, even the insulin receptor (one of many different types of cell receptors) has multiple additional roles in physiological processes within us.
The diagram below 9 gives a brief overview of this complexity (sometimes referred to as pleiotropy – where one gene affects other seemingly unrelated traits).
Insulin through its receptor affects multiple physiological processes in the organism (left) by increasing (green arrows) or decreasing (red arrows) various intracellular metabolic pathways (right).
Time to call the locksmith
All well and good, but if the pancreas doesn’t produce insulin (as in T1D) then our muscle cells don’t get any energy, no matter how much glucose is floating around in the bloodstream, because there’s no key (insulin) to open the lock (insulin receptor in the cell membrane). This is why sufferers of T1D have to have insulin injections (the locksmith), otherwise blood sugar levels would simply rise and rise and eventually result in death. A person with T1D will have to monitor their blood sugar levels very carefully if they’re in the habit of eating bowls of Frosties – a habit which would not be recommended by any medical expert.
When the fat hits the fan
But what about T2D, where there’s still plenty of insulin being released into the bloodstream from the pancreas – at least, until later stages of untreated/unreversed 10 diabetes? If our muscle cells are so full of intramyocellular lipids (fat stored as a result of less-than-ideal dietary habits, where sugary foods like Frosties and high-saturated fat products have been eaten over extended periods of time), the key won’t be able to open the lock – again, no matter how much insulin and glucose might be available. The result is similar to T1D: blood sugar levels can rise and rise. 11
Dr Greger explains this process in more detail in his video, “What Causes Insulin Resistance?” 12 .
Diabesity
The link between obesity and diabetes (so strong now that the term ‘diabesity’ 13 has been coined) can be explained by realising that the fat spilling into the bloodstream from fat cells in obese individuals can get lodged in the very muscle cells we’ve been talking about. This then leads to insulin resistance and the onset of T2D.
So, although Frosties contain very little fat (only 0.6%), if the person eating them is already obese, the blood glucose quickly resulting from their consumption will end up in the bloodstream and find that the muscle cells are already fully or partially blocked by the intracellular fat 14 . Some of the glucose will be stored as further fat deposits, while some will continue to circulate in the bloodstream.
Non-alcoholic fatty liver disease
In T2D, the pancreas has been pumping out more and more insulin in an effort to overcome the fat induced insulin resistance in muscle cells. Over time, these high blood insulin levels can lead to accumulation of fat in the liver – non-alcoholic fatty liver disease (NAPFD).
Before the final diagnosis of T2D, the liver will certainly be protesting, without its owner ever hearing its silent screams. But eventually, this fat build up in the liver will make it, too, resistant to insulin in the same way as it does with the muscles.
Breakfast & the liver
Between meals, a normal liver will constantly be turning its stores of glycogen into glucose, which it then pumps into the blood to keep the brain alive; and when we do eat breakfast, after a night without dietary intake, the insulin released from the meal should turn off liver glucose production. However, if there’s too much fat in the liver, it fails to respond to that breakfast signal.
The fatty liver continues pumping out glucose all day long, on top of whatever we’re eating. The pancreas responds to the high level of blood sugar by releasing more insulin, causing the liver to get fatter and fatter. Meanwhile, fatty muscles (i.e. muscle cells that have been stuffed with surplus fat), within the context of eating too many calories, leads to the fatty liver getting even fattier.
And this all starts beforediabetes is even diagnosed. This is why it’s a mistake to under-estimate the danger of being prediabetic.
Cycle #2
Fatty liver can be fatal and, because our bodies do all they possibly can to keep us alive (in spite of the relentless pressure we may impose on them), the liver tries to offload the fat by dumping it back into the bloodstream in the form of VLDL (very low density lipoprotein). This then finds its way into the beta (or so-called eyelet) cells of the pancreas, making it into a fatty pancreas – thereby destroying the ability of the pancreas to produce insulin. Blood sugar levels go up and up, leading to hyperglycemia – damaging the vessels supplying blood to vital organs, increasing the risk of heart disease, stroke, kidney disease, vision loss and irreversible nerve damage, gangrene, amputations and, of course, death.
Thus, by looking at these two cycles, it’s possible to see how T2D diabetes develops and to understand how it is a condition of excess fat inside our organs.
Final thoughts
Just eating the odd bowl of Frosties isn’t, of course, going to lead to diabesity; but if we tell ourselves that eating such foods “isn’t really all that bad” (they are, after all, fortified with added vitamins and minerals!), then we’re also likely to justify eating a whole load of other processed foods. And it’s the combination of these fatty, sugary, salty, processed foods being eaten over extended periods of time that ends up causing serious diet-related diseases.
Another important aspect is that every time we choose such unhealthy foods, we establish habits and addictions that can keep us locked in to vicious cycles – starting with those silent screams within, but ending up with very apparent indications of harm that’s already been done.
I think I’ll give Mr Kellogg’s offerings a miss.
You may want to have a go at the brief quiz below…
A little more information on carbohydrate metabolism: Not all cells in the body are the same in relation to their requirements for glucose and only glucose. Erythrocytes (red blood cells) and neurones (brain cells) can use only glucose for fuel. This means that the maintenance of blood glucose levels is vital to ensure the provision of a constant energy source to these cells.
Most other cells can also use other sources of fuel (amino acids, fatty acids, glycerol and occasionally nucleic acid) in a process called gluconeogenesis.
So, while some glucose is transported to the liver (to satisfy its own significant energy requirements), and some will be oxidised in other cells around the body, a certain level of glucose has to remain in the circulating blood to maintain the normal blood glucose of about 3.5– 8 mmol/ L (63– 144 mg/ 100 ml). If there is excess glucose above blood level requirements, insulin will convert it to the insoluble polysaccharide, glycogen, in the liver and in skeletal muscles.
Glycogen is the main storage form of glucose in animal cells. In humans, most glycogen is found in the liver (10% of the liver mass), with muscles only containing a relatively low amount (1% of the muscle mass), and small amounts of glycogen also being stored in some glial cells in the brain.
Inside cells, glycogen-formation is a means of storing carbohydrate without upsetting osmotic equilibrium. However, before it can be used to maintain blood levels or provide ATP, it has to be broken down again into its constituent glucose units.
Liver glycogen stores constitute a store of glucose used for liver activity and to maintain the blood glucose level.
Muscle glycogen stores provide glucose requirements of muscle activity.
Glucagon isn’t the only hormone associated with the breakdown of glycogen to glucose, adrenaline (epinephrine) and thyroxine are are also involved. Naturally, if there is an excess of carbohydrate, above that required to maintain blood glucose level and glycogen stores in the tissues, it will be converted to fat and stored in the fat depots around the body.
After looking at the confusion, not just about the best type of breakfast, but about whether breakfast was a good idea in the first place 1 , a recent newspaper article, “Beware the ‘bliss point’ – the sinister reason why you can’t put down your favourite snacks” 2 raised some pertinent points.
Linked to this topic are two books I would strongly recommend: “Salt, Sugar, Fat: How the Food Giants Hooked Us” by Michael Moss 3 , and “The Pleasure Trap: Mastering the Hidden Force That Undermines Health and Happiness” by Doug Lisle & Alan Goldhamer 4 .
Blog Contents
Bliss point & pleasure trap – What’s the problem?
The bliss point is something that food manufacturers employ expert scientists to find so that you become addicted to their foods. Too blunt a way of putting it? Okay, maybe the above-mentioned newspaper article will put a little more flavoursome flesh on the bones.
You may already be aware that we in the UK eat more processed food than any other European nation – around 50.7% of our diet on average, and this figure only appears to be going in one direction – upwards 5 . With the growing interest in veganfoods, many of which are highly processed in an attempt to mimic animal foods like burgers and sausages, even those choosing a plant-based diet may not be able to avoid the bliss point and thus getting caught in the pleasure trap, unless they scrutinise the ingredients lists.
But what’s the bliss point got to do with this? Michael Moss, author of the above-mentioned “Salt, Sugar, Fat: How the Food Giants Hooked Us” says:
“The bliss point is an industry reference to the perfect amount of sugar in products that will get us to not just like those products, but to want more and more…It’s a specific reference to sugar, although it’s been used more broadly to refer to the incredible allure that processed foods have.”
So, when we casually joke that we can’t resist certain foods (from biscuits and ice-cream to crisps and cheesy/meaty ready-meals), the truth is closer than we think – brilliant scientific minds are employed specifically to ensure that our brains make it virtually impossible for us to resist the temptation to eat more than we probably know is good for us.
Salt, fat and sugar
When salt, fat (whether in solid form like lard and butter or liquid like sunflower or olive oil) and sugar are combined, your brain doesn’t stand a chance against the pleasure signals your tongue will send it.
In nature, these three are rarely – if ever – found together in any natural food. Yet, our animal brains have been programmed over millions of years of evolution to fill up on fatty and sugary foods whenever we were lucky enough to find them. This would normally occur seasonally – picking fruits in summer and autumn, or coming across a beehive full of energy-rich, sweet honey.
But nowadays, we’re surrounded by these “Frankenfoods” 6 , which ‘pull us back in’. And these Big Food guys and gals are pretty cute – so that, even when you’ve selected what you think is the healthy low-fat, non-gluten, organic, locally-sourced and sustainable ready meal, they’ll already have ensured that whatever addictive element was reduced in quantity, was replaced by an increase in another equally-addictive element.
We’ve been processed just like the food!
There’s no doubt that most of us consider that we are doing our best to eat more health-consciously; but it’s really an uphill battle when you’re fighting against Big Food and their hunger for making huge profits from cheap ingredients – apparently with little regard for the devastating health implications for the unwitting consumer, while virtue-signalling the food’s health benefits. All efforts to change the “profit over health” bias within major food manufacturing, even by leading-lights such as Hugh Fearnley-Whittingstall, appear to produce little more than token gestures from the likes of Kellogg’s and Nestlé 78 .
Voting with your feet
This is all well and good if you know which direction to go. However, even when we watch documentaries or read articles that reveal these industry techniques, aimed at making us addicted to their products, we still unconsciously reach out for that bag of crisps or the chocolate Hobnobs. With this onslaught of industry influence, no matter how healthily we try to eat, few of us are likely to discover the route to a truly healthy, life-long plant-based diet, free of all the pleasure traps and bliss points – at least, when the only information we receive comes via clever media trickery.
So are plant-based foods tasteless?
It could be argued that anything which compels you to consume something, even though you implicitly know that it’s bad for you, is an addiction with certain negative health connotations. People don’t smoke tobacco, inject heroin or drink excess amounts of alcohol without being aware both that it’s bad for them and that they find it really difficult to stop. There appears to be little difference between these forms of addiction and processed food.
With unadulterated plant foods, your body will not allow you to reach a point of no return – where you are so addicted that you consume more of something than your body knows is good for you. When you eat a food that your body recognises as food, with all the natural combination of fibre, water, macro- and micro-nutrients, there’s a perfect alignment between the amount your stomach contains and the amount your brain thinks has been consumed. A previous blog 1 showed that this alignment does not exist when it comes to highly calorific, salty/sugary/fatty processed foods.
As for whether or not plant-foods lack flavour, our taste buds (and brain) become accustomed to the natural flavours of natural foods. An imperceptible shift occurs in both our expectations of what food will provide and in the satisfaction we derive from it. After only a short period of time (often only a number of days) of being freed-up from the overpowering saltiness, fattiness and sweetness of processed foods, our taste buds normalise and the true flavours emerge.
It’s true that a memory of previously-eaten foods will remain somewhere in the recesses of the brain, much like an ex-smoker will always have some part of his or her brain that’s still drawn to the memories of social or psychological aspects of the addiction – but, the memories are invariably selective in nature. When one has the occasional yearning for a blow-out meal of fish and chips or a Double WhopperMeal, it’s so easy – I know – to remember how wonderful they tasted – even causing us to physically salivate, much like Pavlov’s dogs 10 – but, of course, without immediately recalling how stuffed and ill we may have felt immediately afterwards, and how we promised not to eat such food ever again.
Cravings – a thing of the past?
It can come as quite a surprise when you find that eating a WFPB begins to free you up from food cravings. When you’re hungry, you eat. Plants, being rich in nutrients and low in calories11 , fill you up more than foods high in calories and low in nutrients.
The whole is greater than the sum of its parts
One important point to recognise is that you wouldn’t be able to consume as much of a given food if salt, sugar or fat were added individually without the others. It’s the combination of these three that’s able to fool your brain.
Would you let a stranger give your child a cigarette?
Moss, says: “There’s nothing more important than the bliss point to understand how we became so overly dependent on processed foods.” Dr Joel Fuhrman’s excellent book, “Fast Food Genocide: How Processed Food Is Killing Us and What We Can Do About It” 12 , provides such a clear analysis of this situation that I’m obliged to quote a fair chunk below:
“Consuming fast food is legal and socially acceptable. But these foods, rich in added sweeteners, salt, oils, and artificial flavoring (called “highly palatable foods” by scientists) have addictive properties. Eating a little makes you want more. Overeating and substance-drug abuse share important common characteristics, including tolerance (needing greater amounts over time to reach the same ‘high”), unsuccessful efforts to cut back on consumption, and use of the substance despite negative consequences. 13
Sugar-izing all foods to reach the “bliss point” that maximises pleasure (and purchases), leads to a gradual deadening of the taste buds. Over time, this has two negative consequences: first, you crave more and more sugar; and second, the level of sweetness in natural foods (such as berries and carrots) no longer has any appeal. Children raised on fast food meals, soda, and frequent junk food treats do not like fruits and vegetables. Why? Because they can hardly taste these foods. Their taste buds have been shut down by excess salt and sugar and simply can’t register the nuances of flavors in real food.
Fast food prevents you from tasting the naturally delicious flavors of fruits and vegetables; therefore, the very foods that provide the body with the necessary nutrients to thrive and live a long, healthy life are made less desirable by human-made processed foods designed to cultivate addictive consumption.
Feeding sweetened soda, doughnuts, cake, and junk food to children is practically the same as handing them a shot of whiskey or lighting up a cigarette for them. There is just a small degree of difference between one addictive, dangerous substance and another. The same brain centers are stimulated by cocaine, narcotics, and super-sweetened foods. It is debatable which is more deadly, as so many people eat super-sweetened foods multiple times a day every day.” 14
Where did the bliss come from?
The term ‘bliss point’ was first coined by the market researcher and psychophysicist Howard Moskowitz around the 1970’s. Since that time, he worked with Big Food to optimise junk foods as wide-ranging as soft drinks, soups, salad dressings and pasta sauces.
Mr Kellogg, way back in the 19th century, started the taste for processed breakfast cereals, which have become further contaminated with loads of sugar, artificial sweeteners, colourings and flavourings over the past decades. But it was in the 1970’s and 1980’s that “extraordinary science to perfect our taste reaction” really took off, according to Michael Moss, with the food scientists engineering such terms as “moreishness,” “craveability”, “snackability”, “mouthfeel”, “flavour burst”, etc. No coincidence, then, that this heralded the start of the massive rise in obesity levels and other non-communicable diseases 1516 .
Intentional or not?
Do the food manufacturers do all this on purpose in order to make us ill? I’ll let you decide that – although you may have to research Big Food’s links to Big Pharma to get a full picture!
However, it’s hard to consider it an accident when if you look at the amount of sugar, fat and salt they pile into every processed food – from ready meals to crisps, and from loaves of bread to children’s yogurts – especially when there is a mountain of scientific studies showing the devastating impact such foods have on human health.
The Telegraph article mentions a really cute technique that food scientists call “vanishing caloric density“, specifically in relation to the supposedly light snack, “Cheesy Puffs“:
“The human body…is pretty good at detecting calories. After all, they were once our primary concern. But clever brains at food corporations can get around that. Cheese puffs are a highly fatty, salty (and often sugary) snack. But when they melt in the mouth, our brain thinks the calories disappear along with the puff. Clever.”
Discussing the book, “The Pleasure Trap“, the TrueNorth Newsletter says: “people who are chronically overweight, miserable, or junk food junkies aren’t that way because they’re lazy, undisciplined, or stuck with bad genes. They reveal that they are victims of a primal dilemma that harkens back to our prehistoric past called The Pleasure Trap..” 17
The innate incentives from our ancient ancestors, which they call The Motivational Triad consists of three elements:
the pursuit of pleasure
the avoidance of pain, and
the conservation of energy
The newsletter continues: “Unfortunately, in present day America’s convenience-centric, excess-oriented culture where fast food, recreational drugs, and sedentary shopping have become the norm, these basic instincts that once successfully insured the survival and reproduction of man many millennia ago, no longer serve us well. In fact, it’s our unknowing enslavement to this internal, biological force embedded in the collective memory of our species that is undermining our health and happiness today.”
Final thoughts
So what’s the main benefit of switching to a WFPB diet?
The answer to this question could probably be summed up in just one word:
FREEDOM.
Freedom from the pleasure trap and freedom from enslavement by that boring cycle of bliss point-chasing and bliss point-regretting.
And it doesn’t stop there. This enlightened self-interest will also play a part in :
Mental and physical health – your body and mind will ‘thank you’ for choosing arguably the most nutritious and healthy diet18
Environmental & animal welfare – your dietary choices will help to produce immediate and remarkable positive benefits for the environment and the protection of other animal species on our planet 19
You may have come across warnings about consuming foods high in nitrates and/or nitrites, with respect to both animal- and plant-based foods. But what does the science say? Whilst previous blogs have touched on this subject – specifically in relation to chewing vs juicing1 and whether athletic performance is affected by nitrate consumption 2 – here, the subject of dietary nitrates and nitrites is covered in more depth, to provide some clarity on which foods are to be avoided and which are to be embraced.
Blog Contents
Nitric Oxide – The Good Stuff
Really, this is all about a vital molecule called nitric oxide (with the chemical formula NO). In any list of the most important compounds within the human body, NO is right up there.
It’s so important because it gets involved in pretty much every single organ system within the body and has a central role as a major and powerful vasodilator. This means that it makes blood vessels wider – of immense importance in allowing the blood to flow without the heart having to strain.
There are a wide range of common diseases associated with insufficient NO, including:
The list goes on and on…really, it’s hard to over-estimate the importance of NO for human health.
But what have nitrates and nitrites got to do with nitric oxide?
Nitrates, Nitrites & Nitric Oxide
The above diagram 18 basically indicates that the body converts dietary nitrates to nitrites and then to NO (as well as to ammonia) 19 . During this process, an enzyme connected to the non-essential amino acid L-arginine (also just known as arginine) is required in order to produce NO from the nitrites. L-arginine is called ‘non-essential’ (or, more specifically, a ‘conditionally indispensable amino acid’) because, although it can be derived from foods, the body can also produce a certain amount of it. 20
L-arginine is found in many protein-containing foods, both animal- and plant-based21 .
Increasing age, smoking, high cholesterol, inflammation, dietary deficiencies and other factors can negatively affect the functioning of the enzyme required for this conversion of L-arginine to NO. And the problem of insufficient L-arginine is not solved by taking L-arginine supplements – indeed, L-arginine supplements have been shown, not only to be ineffective and even cause less NO to be produced 23 , but such supplements have led to increased mortality when given to patients who have had heart attacks :
“L-arginine, when added to standard postinfarction therapies, does not improve vascular stiffness measurements or ejection fraction and may be associated with higher postinfarction mortality. L-arginine should not be recommended following acute myocardial infarction.” 24 .
So what do we need to do to ensure that we have optimal NO levels?
First – A Bit of NO History
In 1987, Bob Furchgott25 was the first to propose that NO was the EDRF (endothelium-derived relaxing factor) – i.e. that NO was the stuff responsible for the observed dilation of blood vessels, as well as a range of other vital physiological processes. Thus, NO is a relative newcomer to pharmacology. However, its impact was so significant that Bob Furchgott and his two collaborators, Louis J Ignarro and Ferid Murad, received the Nobel Prize in Physiology for its discovery.
Since then, hundreds of thousands of papers have been published with reference to NO – both in respect of NO as the endothelium-derived relaxing factor, as well as the role of L-arginine in NO synthesis.
During the time since 1987, the significance of the L-arginine:NO pathway has increased considerably – in relation to both the importance and the range of physiological roles this pathway plays. Roles which include:
maintenance of vascular tone
neurotransmitter function regulation in both the central and peripheral nervous systems
mediation of cellular defence
interaction within mitochondrial systems to:
regulate cell respiration, and
augment generation of reactive oxygen species, thereby
During this time, and until fairly recently, there was a particular concern about a potential increase in cancer risk from dietary nitrates and nitrites. This concern was accompanied by (and perhaps, to some extent, based on) the mistaken belief that the enzyme responsible for synthesising L-arginine within the body was the only pathway to produce NO in humans.
However, it’s been shown that when we ingest dietary nitrate, bacteria in the oral saliva convert it to nitrite. This nitrite is then swallowed and gets further converted into NO within the stomach, blood vessels and tissues 2728 .
Mouthwashes, Antibiotics, Spitting & NO
We’ve looked previously 29 at the important role played by the bacteria in our mouths (the oral microbiome), and how it differs between meat- and plant-eaters. It’s important to stress that these oral bacteria are absolutely essential for the production of NO from our foods. Indeed, they are vital for this process, since humans can’t convert dietary nitrate to nitrite – it’s the bacteria living in our mouths that do the conversion.
So, predictably enough, it’s been shown 3031 that, if you kill these oral bacteria by using an antibacterial mouthwash or taking antibiotics, the production of NO from dietary nitrate can stop completely. Additionally, if you spit a lot, you can deplete the bacterial concentration in your mouth, and this has a significant effect on nitrate conversion 28 .
Antacids & NO
Stomach acid also provides another important step in the production of NO from dietary nitrate 32 . Therefore, reducing the concentration of stomach acid by taking certain medication, including antacids and acid-reducing medications (such as Losec 33 ) can also decrease NO production and, thus, diminish its protective benefits 27 .
Quantity Matters
Today, dietary nitrate is understood as a highly significant precursor to NO in a dose-dependent manner34 . So, the more nitrate consumed, the more NO becomes available in the body. There are, of course, upper limits, but these are only when nitrates are consumed in very large quantities, and this is unlikely (if even possible) from eating a WFPB diet – unless you’re unwise enough to take supplements.
Plant Nitrates vs Animal Nitrites
Plants are the primary source of dietary nitrates, while processed/cured meats are the primary sources of dietary nitrites (used as preservatives). It will comes as no surprise that the latter have a different impact on human health than the former.
Ingesting nitrates in plants increases NO and provides protective and healing benefits for a wide range of diseases characterised by insufficient NO (see the above list).
Ingesting nitrites in processed and cured meats (bacon, frankfurters, etc) can cause the nitrites to react with the amino acids, fat and haem iron already present within the meat, resulting in the formation of harmful substances before the meat is even cooked or eaten 3536 .
A previous blog 37 went into more detail on how meat preservation methods have led to such foods being classified as Group 1 carcinogens, along with tobacco and asbestos.
When nitrites are consumed in animal foods, they can form nitrosamines3839 – one of the carcinogenic agents also present in cigarette smoke. Nitrosamines in processed meats (smoked, canned and preserved), as well as in grilled meats, are formed from nitrites in the absence of phytonutrients and antioxidants found in plant foods. “Just a few hot dogs may contain the carcinogenic nitrosamine load of a pack of cigarettes. In fact, just the smell of frying bacon even contains nitrosamines.” 40 Indeed, whenever you consume a diet high in animal foods (whether it’s processed meats or organically-produced eggs or dairy), you’re consuming nitrites in the absence of the phytochemicals and antioxidants that only plants contain.
Athletic Performance, NO & ATP
A previous blog, which looked at the effects of NO on athletes2 , emphasised how important NO is for optimal athletic performance and recovery. Basically, dietary nitrate in plant foods increases the diameter of blood vessels, thereby increasing the volume of blood moved around the body with each heartbeat. This increases oxygen production to the muscles and thus increases muscle strength.
Another aspect of the relationship of NO to physical activity is ATP (adenosine triphosphate) . ATP is produced when the food we’ve eaten is metabolised in the presence of oxygen 41 . ATP is within every cell of our bodies and produces the energy we need to survive and function. The more oxygen within our red blood cells, the more ATP can be produced and, thereby, the more energy we can have available to us. However, it’s not just a matter of being an athlete with bigger lungs that facilitates this; recent research has shown 42 that dietary nitrate can actually decrease the amount of oxygen you need in order to produce sufficient ATP – that is, more work can be performed using the same amount of oxygen inhaled. Dietary intake of nitrates appears to be particularly effective for short-term, high-intensity rather than long-term, less intensive exercise.
Dietary Nitrate & Mitochondria
Furthermore, it appears 43 that dietary nitrate also improves the efficiency of our mitochondria (the energy-producing powerhouses within every human cell). Thus, increased nitrate consumption can have significance for athletes, people who live at high altitudes (where oxygen levels are lower in the air), and people with certain oxygen-limited diseases (e.g. lung disease or sleep disorders) .
Research has shown 44 particular benefits of nitrate consumption for those individuals who have lower fitness levels and/or impairments related to their muscles, heart and/or lungs, for instance in cases of non-ischaemic, dilated cardiomyopathy45 , COPD46 , heart failure47 , and peripheral artery disease48 .
Blood Pressure & NO
There are few conditions that cause more chronic illness and early deaths than hypertension. And the increase in the number of people affected is clearly associated with the increase in prevalence of the Western diet – richer in animal foods and processed junk than any time in human history.
And it’s all connected to the function of NO. Since two of NO’s major functions are to maintain the health of the single layer of delicate endothelial cells lining our blood vessels, and to ensure that our blood vessels dilate effectively, any reduction in production of NO is bound to result in damage to the integrity and flexibility of the vessels.
increased dietary nitrates = increased nitrite production in the body
increased nitrite production in the body = increased NO
increased NO = decreased blood pressure
decreased NO = increased blood pressure
Even in early studies with young, healthy individuals, it’s been shown 4950 that dietary nitrate-consumption decreases their blood pressure. More recent research also demonstrates 515253 how it can also decrease blood pressure in those more at-risk populations who already have high blood pressure. One study 54 concluded: “an additional strategy, based on intake of nitrate-rich vegetables, may prove to be both cost-effective, affordable and favourable for a public health approach to hypertension.” Another study 55 showed how chronic OSA (obstructive sleep apnea) could be effectively treated by reducing blood pressure as a result of simply eating more dietary nitrates in plant-based foods. And research is starting to suggest 56 that brain disorders such as dementia, Alzheimer’s disease, etc may be helped by dietary nitrates helping to increase blood flow to the brain.
It took some time for scientists to be convinced that eating your veggies could really increase NO when other conventional therapies had continually failed to do so. But now, the sheer weight of research data supports this view – as one editor of an eminent journal stated 57 back in 2008: “Mother was right: eat your vegetables and do not spit!”
Long-Term vs Short-Term
As with most aspects of nutrition, doing the right thing for longer is more effective than doing it for shorter periods of time. This is no different with vegetable-consumption and NO production. It appears that the longer you eat a plant-based diet, the more beneficial the effects on your health. It makes sense, therefore, that transitioning to a life-long WFPB diet, rather than merely opting for a short period of relief from animal proteins (for instance, during Veganuary) and processed junk, is the way to enjoy maximum life-long benefits.
How Safe Is Dietary Nitrate?
Ingesting nitrates when they are inside vegetables is extremely safe, being that they are combined with fibre, antioxidants and phytochemicals. Having said this, infants under the age of three months should not be given dietary nitrates – that is, not fed vegetables 58 . This shouldn’t even be an issue since, as we saw in a highly-detailed previous blog on Vegan Pregnancy & Parenting 59 , all babies of this age should only be receiving breast milk or, if that is not available, appropriate formula milk.
Also, for those taking particular medications (including blood-thinning drugs like Warfarin), the high levels of vitamin K (phylloquinone) in green vegetables can be a potential issue, since vitamin K’s blood-clotting action can reduce the required actions of the prescribed drug. As Dr Greger says 60 : “In fact dark green leafies are so packed with vitamin K that if you’re on the drug coumadin (warfarin), a drug that works by poisoning vitamin K metabolism, you have to closely work with your physician to titrate the dose to your greens intake so as to not undermine the drug’s effectiveness!”
How To Increase Nitrate Intake
Although there is some variation in levels (depending on plant type and the quality of the soil used for growing), it’s important to understand that all whole plant foods contain nitrates. Whilst around 85% of nitrates will come from the plants you eat, around 15% is actually contained in the water you drink 61 .
Green, Leafy Veg
Research indicates 6263 that green, leafy veg have the highest levels of nitrates:
rocket (arugula in the US)
cabbage
lettuce
chard
beetroot and rhubarb have moderate amounts
carrots and other veg contain lesser amounts
USA & European Nitrate Consumption
Surveys of dietary habits in the US and Europe show 6451low levels of daily nitrate intake (~0.5-3 mmol/day), which is consistent with the low levels of vegetable consumption. All diets which tend to contain more vegetables (such as Japanese diets, the DASH diet, vegetarian and vegan diets), all show 65 a higher amount of nitrate intake (~20 mmol/day) than standard Western diets.
Regular & Sufficient Nitrates
The positive effects of dietary nitrate don’t last for ever. The peak effectiveness appears to be 28 at around three hours after consumption. There’s still some benefit after this point, but after 24 hours the effect of the nitrate is virtually nil. Thus, the ideal diet would consist of nitrate-rich foods being consumed at least a couple of times each day.
In terms of nitrate quantity, one study suggests 66 that 8.4-16.8 mmol/day produces the greatest improvement in NO utilisation (and, hence, in exercise performance), while 4.2 mmol/day produces little or no effect and anything above 16.8 mmol/day appears to achieve no additional benefits. The suggestion is that maximum benefit is achieved with ~10 mmol/day – quite manageable by eating a moderate amount of varied plant foods (green leafy veg, beetroot, rhubarb, etc). Exercise is also reported to increase NO production.
Final thoughts
Whatever you may have heard to the contrary, the consistent scientific consensus is that green, leafy veg are one of the healthiest foods on the planet for humans, and many authorities maintain 676828 that the NO-producing nitrates in those veg accounts for a lot of these health benefits. 69
Finally, how better to finish than a short video by Dr Michael Greger?
More on L-arginine and NO synthesis: Another amino acid, L-citrulline, found in watermelons and also produced in the body, is an endogenous precursor for L-arginine. The family of enzymes involved in L-arginine synthesis – the NO synthases (NOSs, EC 1.14.13.39) – catalyse the oxidation of L-arginine (Arg) to NO and l-citrulline, with NADPH and O2 serving as cosubstrates (Alderton, R. K., Cooper, C. E. & Knowles, R. G. (2001) Nitric oxide synthases: structure, function and inhibition. Biochem. J. 357(pt. 3):593–615.). The NOSs first hydroxylate a terminal guanidino nitrogen of Arg to generate N-hydroxy-l-arginine (NOHA) as an enzyme-bound intermediate. NOHA is then oxidized further by the enzyme to generate NO plus l-citrulline. [↩]
Special thanks to Conor Kerley PhD, writing on behalf of CNS, for his article “Nitric Oxide & Dietary Nitrate: Another Reason to Eat Your Vegetables”, December 13, 2017. [↩]
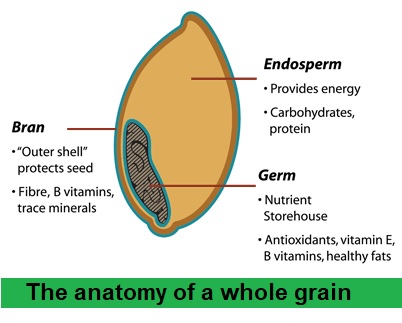


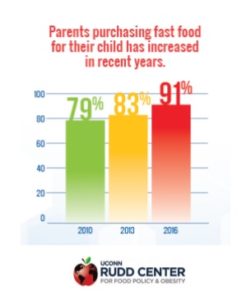 Just two words can sum up the major cause of FUN: ‘fast’ and ‘food’. Whether from take-aways, restaurants or supermarket shelves, fast food provides that perfect storm of high calories/low nutrients for children and adults alike.
Just two words can sum up the major cause of FUN: ‘fast’ and ‘food’. Whether from take-aways, restaurants or supermarket shelves, fast food provides that perfect storm of high calories/low nutrients for children and adults alike.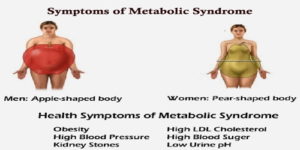 As our populations reach advanced age,
As our populations reach advanced age, 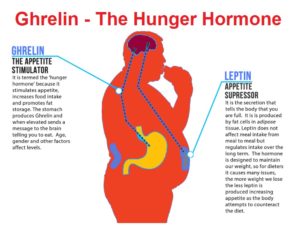
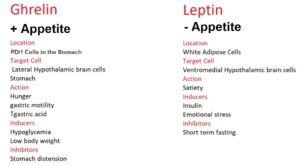
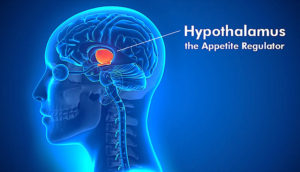 They are both
They are both 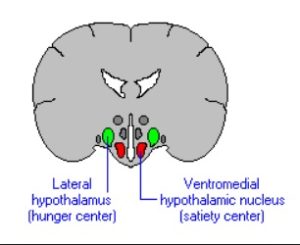 Ghrelin and leptin act on different parts (receptors) within the hypothalamus.
Ghrelin and leptin act on different parts (receptors) within the hypothalamus.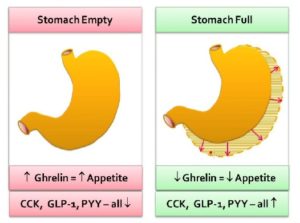
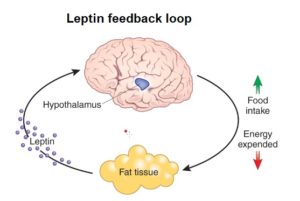 Leptin, on the other hand, is primarily produced by white adipose tissue.
Leptin, on the other hand, is primarily produced by white adipose tissue.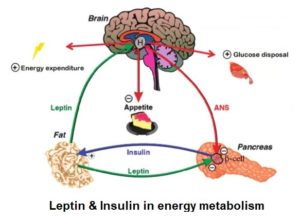
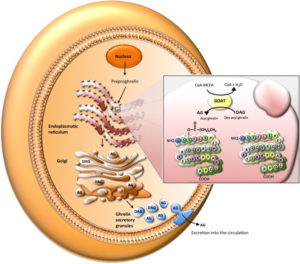
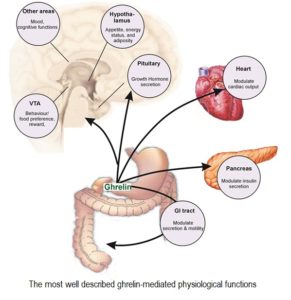 The discovery of the GOAT enzyme revealed that ghrelin is involved in many additional physiological functions, ranging from regulation of the immune and cardiovascular systems, up-regulation of insulin-like growth factor (IGF-1), to a dominant role in the gastrointestinal system and involvement in gastric emptying and
The discovery of the GOAT enzyme revealed that ghrelin is involved in many additional physiological functions, ranging from regulation of the immune and cardiovascular systems, up-regulation of insulin-like growth factor (IGF-1), to a dominant role in the gastrointestinal system and involvement in gastric emptying and 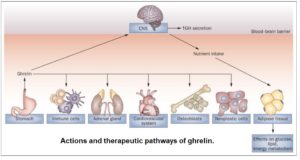 As can be seen in the diagram, ghrelin affects multiple systems. Whilst being secreted mainly by the stomach, it has effects in multiple areas, including the CNS (central nervous system), the immune system, the adrenal gland and the cardiovascular system. It can also affect the proliferation of
As can be seen in the diagram, ghrelin affects multiple systems. Whilst being secreted mainly by the stomach, it has effects in multiple areas, including the CNS (central nervous system), the immune system, the adrenal gland and the cardiovascular system. It can also affect the proliferation of 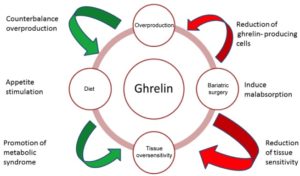
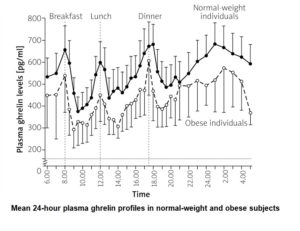
 Ghrelin, as stated above, causes the release of growth hormone (hence the proposed origin of its name – Growth Hormone Release Inducing hormone). The relationships between obesity, adipose tissue, GH and ghrelin make an already complex situation even more complex.
Ghrelin, as stated above, causes the release of growth hormone (hence the proposed origin of its name – Growth Hormone Release Inducing hormone). The relationships between obesity, adipose tissue, GH and ghrelin make an already complex situation even more complex.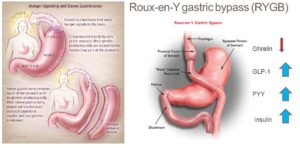
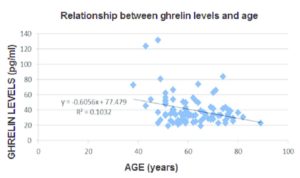 The adjacent graph
The adjacent graph 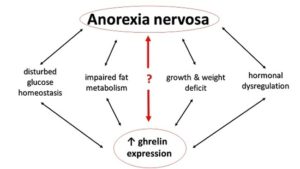 Due to the proven relationship of ghrelin with appetite, researchers are also investigating the potential connection of ghrelin to anorexia. Insight into the modification of the endogenous ghrelin system seems to be promising not only for the control of obesity, but also for the management of clinically significant anorexia and pathological weight reduction.
Due to the proven relationship of ghrelin with appetite, researchers are also investigating the potential connection of ghrelin to anorexia. Insight into the modification of the endogenous ghrelin system seems to be promising not only for the control of obesity, but also for the management of clinically significant anorexia and pathological weight reduction.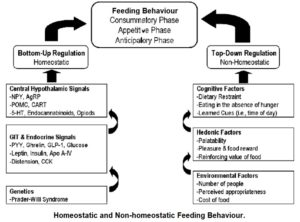 Anorexia nervosa,
Anorexia nervosa, 
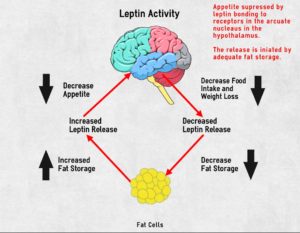
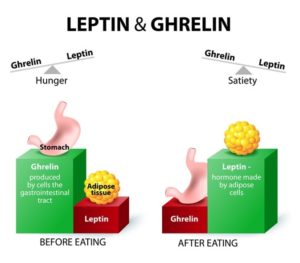
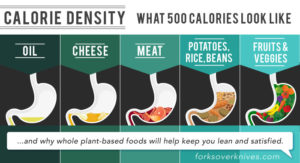
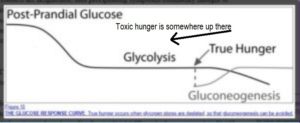





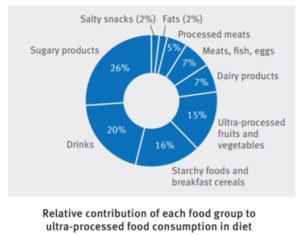

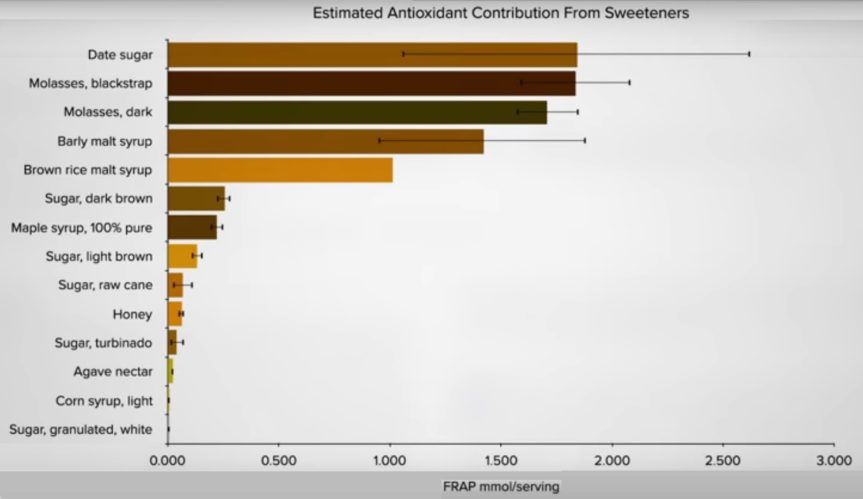
 So what? Isn’t ammonia an alkaline? And previous blogs
So what? Isn’t ammonia an alkaline? And previous blogs 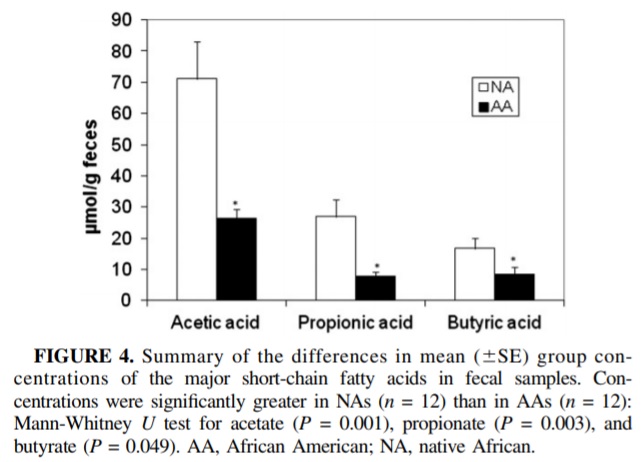 A 2013 study
A 2013 study 
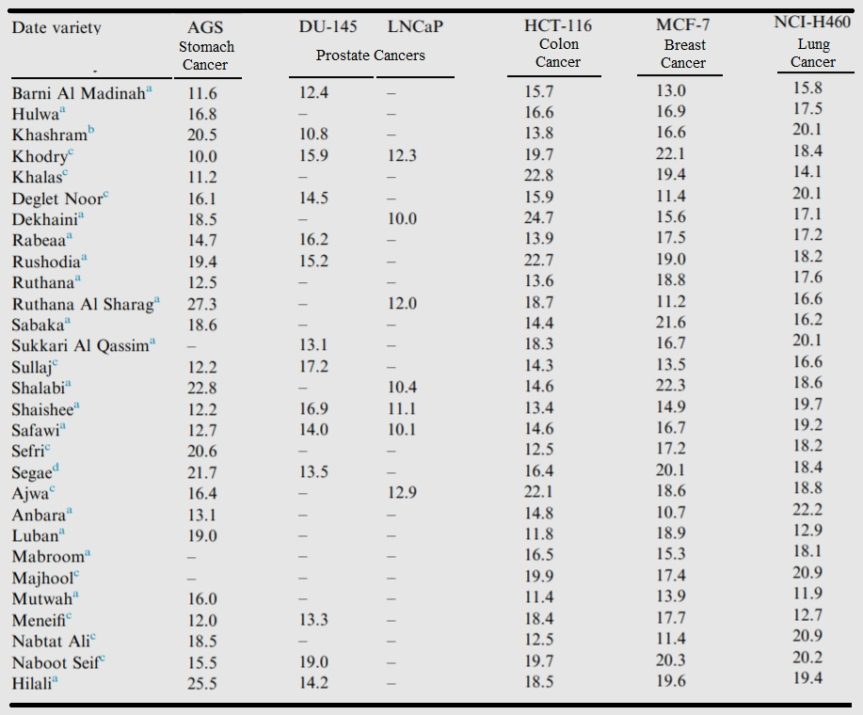


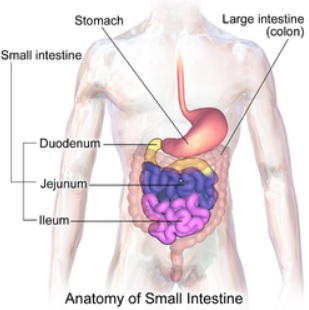 As soon as Frosties enter the mouth, the carbohydrate-digesting enzyme amylase produced in saliva starts to break down the sucrose into its two monosaccharides, glucose and fructose, and the lump of food in the mouth is then referred to as a ‘bolus’.
As soon as Frosties enter the mouth, the carbohydrate-digesting enzyme amylase produced in saliva starts to break down the sucrose into its two monosaccharides, glucose and fructose, and the lump of food in the mouth is then referred to as a ‘bolus’.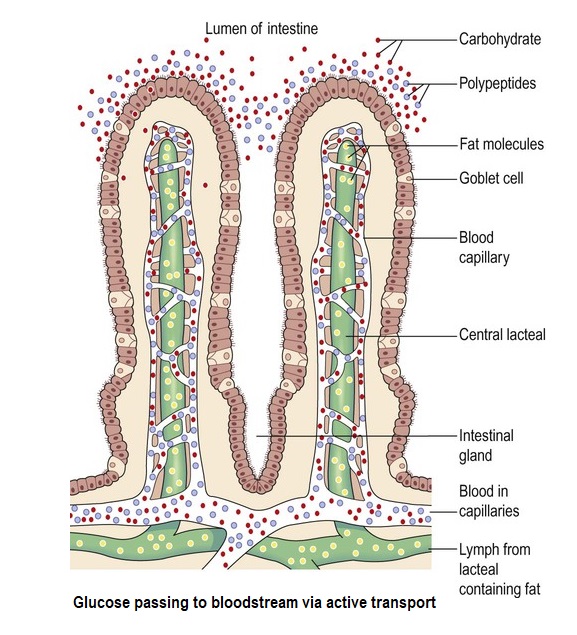 A signal then passes to the pancreas for it to release pancreatic amylase along a duct and into the duodenum.
A signal then passes to the pancreas for it to release pancreatic amylase along a duct and into the duodenum.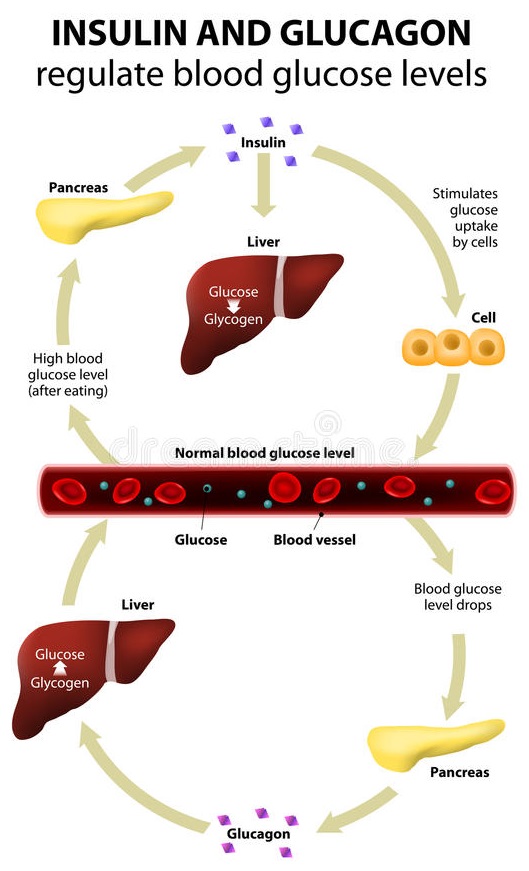 Once the glucose levels rise in the bloodstream, the beta cells of the islets of Langerhans within the pancreas detect this increase and release the hormone, insulin – in healthy individuals, that is.
Once the glucose levels rise in the bloodstream, the beta cells of the islets of Langerhans within the pancreas detect this increase and release the hormone, insulin – in healthy individuals, that is.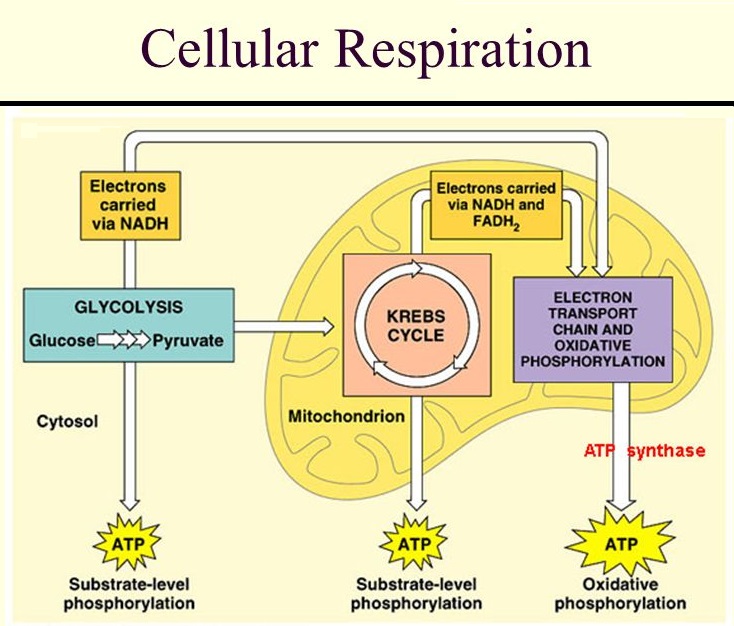 In our scenario, the sugar in the Frosties has been converted into glucose and has ended up in the bloodstream. Insulin’s main job now is to get that glucose into the body’s cells. If it does so successfully – and this is the big IF when it comes to those with T2D – the glucose is oxidised in the cells (that is, the glucose combines chemically with oxygen) and becomes a source of energy. This intracellular energy-production process is known as ‘cellular respiration’.
In our scenario, the sugar in the Frosties has been converted into glucose and has ended up in the bloodstream. Insulin’s main job now is to get that glucose into the body’s cells. If it does so successfully – and this is the big IF when it comes to those with T2D – the glucose is oxidised in the cells (that is, the glucose combines chemically with oxygen) and becomes a source of energy. This intracellular energy-production process is known as ‘cellular respiration’. If glycogen reserves in the liver are saturated, the excess glucose gets converted into fat for long-term storage in the adipose (fat) tissues – beneath the skin (subcutaneous fat), around internal organs (visceral fat) and in bone marrow (yellow bone marrow).
If glycogen reserves in the liver are saturated, the excess glucose gets converted into fat for long-term storage in the adipose (fat) tissues – beneath the skin (subcutaneous fat), around internal organs (visceral fat) and in bone marrow (yellow bone marrow).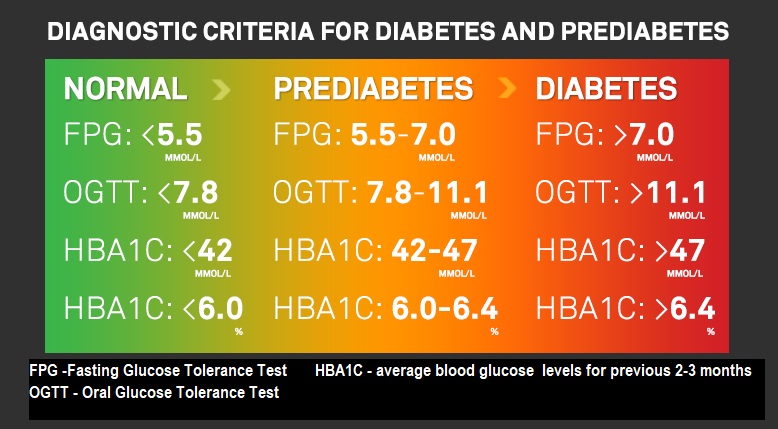
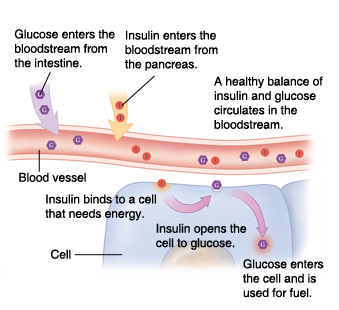
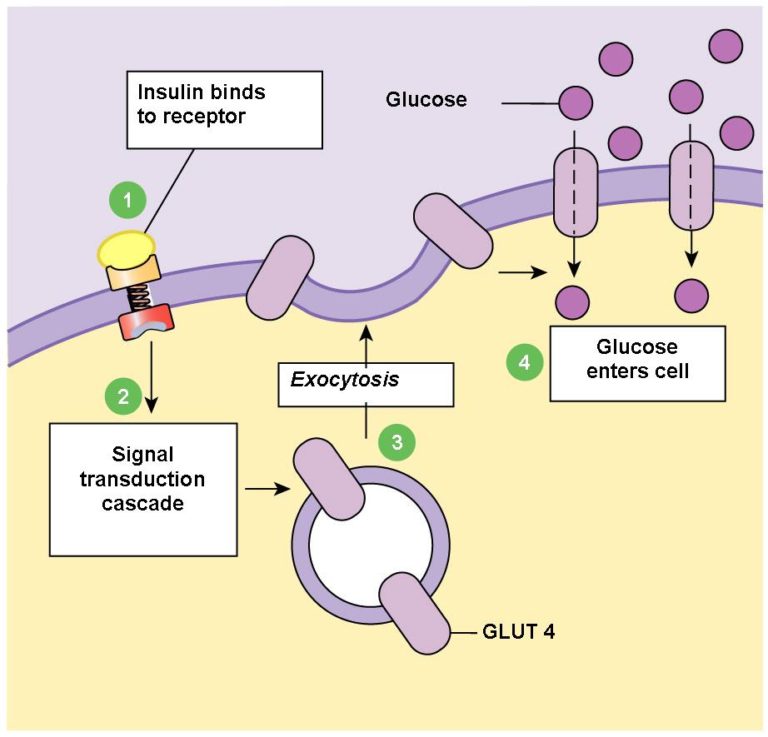
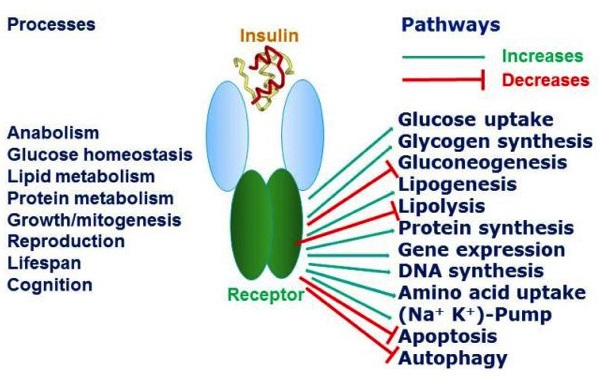
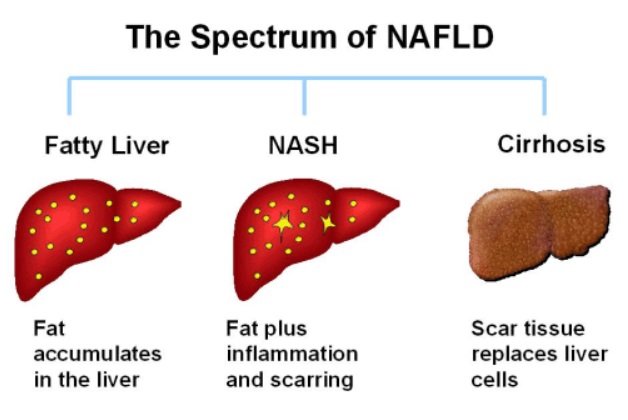 In T2D, the pancreas has been pumping out more and more insulin in an effort to overcome the fat induced insulin resistance in muscle cells. Over time, these high blood insulin levels can lead to accumulation of fat in the liver – non-alcoholic fatty liver disease (NAPFD).
In T2D, the pancreas has been pumping out more and more insulin in an effort to overcome the fat induced insulin resistance in muscle cells. Over time, these high blood insulin levels can lead to accumulation of fat in the liver – non-alcoholic fatty liver disease (NAPFD). Source:
Source: 
 You may already be aware that we in the UK eat more processed food than any other European nation – around 50.7% of our diet on average, and this figure only appears to be going in one direction – upwards
You may already be aware that we in the UK eat more processed food than any other European nation – around 50.7% of our diet on average, and this figure only appears to be going in one direction – upwards 
 It’s true that a memory of previously-eaten foods will remain somewhere in the recesses of the brain, much like an ex-smoker will always have some part of his or her brain that’s still drawn to the memories of social or psychological aspects of the addiction – but, the memories are invariably selective in nature. When one has the occasional yearning for a blow-out meal of fish and chips or a Double Whopper Meal, it’s so easy – I know – to remember how wonderful they tasted – even causing us to physically salivate, much like Pavlov’s dogs
It’s true that a memory of previously-eaten foods will remain somewhere in the recesses of the brain, much like an ex-smoker will always have some part of his or her brain that’s still drawn to the memories of social or psychological aspects of the addiction – but, the memories are invariably selective in nature. When one has the occasional yearning for a blow-out meal of fish and chips or a Double Whopper Meal, it’s so easy – I know – to remember how wonderful they tasted – even causing us to physically salivate, much like Pavlov’s dogs 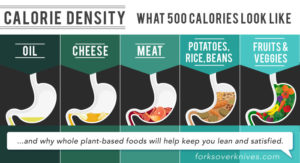
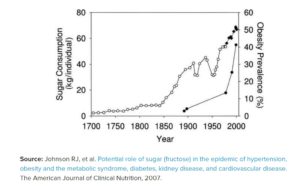 Mr Kellogg, way back in the 19th century, started the taste for processed breakfast cereals, which have become further contaminated with loads of sugar, artificial sweeteners, colourings and flavourings over the past decades. But it was in the 1970’s and 1980’s that “extraordinary science to perfect our taste reaction” really took off, according to Michael Moss, with the food scientists engineering such terms as “moreishness,” “craveability”, “snackability”, “mouthfeel”, “flavour burst”, etc. No coincidence, then, that this heralded the start of the massive rise in obesity levels and other non-communicable diseases
Mr Kellogg, way back in the 19th century, started the taste for processed breakfast cereals, which have become further contaminated with loads of sugar, artificial sweeteners, colourings and flavourings over the past decades. But it was in the 1970’s and 1980’s that “extraordinary science to perfect our taste reaction” really took off, according to Michael Moss, with the food scientists engineering such terms as “moreishness,” “craveability”, “snackability”, “mouthfeel”, “flavour burst”, etc. No coincidence, then, that this heralded the start of the massive rise in obesity levels and other non-communicable diseases  Do the food manufacturers do all this on purpose in order to make us ill? I’ll let you decide that – although you may have to research Big Food’s links to Big Pharma to get a full picture!
Do the food manufacturers do all this on purpose in order to make us ill? I’ll let you decide that – although you may have to research Big Food’s links to Big Pharma to get a full picture!