Dr Joel Fuhrman reverses many chronic diseases – not with medications, radiotherapy or invasive surgical procedures like stents, angioplasty or gastric bands – but simply through changing his patients’ diets.
He created the Nutritarian diet, an eating plan that incorporates the latest advances in nutritional science. At the heart of this diet is the simple health equation, H=N/C.
This equation expresses the concept that your health (H) is predicted by your nutrient intake (N) divided by your calorie intake (C). His ANDI (Aggregate Nutrient Density Index) scoring system, which measures the relative nutrient density of common foods, has helped millions of people to eat an anti-cancer, anti-chronic disease diet.
The aim is to get as high a score as possible. Each food has a given value of between 0 and 1000 per calorie.
Examples
(Refer to chart below for individual food values.)
If you eat 300 calories of food with low nutritional value (let’s say 100 calories each of white pasta, cheddar cheese and olive oil), as you will see from the chart below, these would have individual ANDI values per calorie of 11, 11 and 10 respectively. Add these together and you get 32. Multiplying by 100 calories (the amount of each consumed) gives 3200. Divide this by 300 (the total number of calories) and you get a total ANDI score of 10.7.
If, however, you eat 300 calories of food with high nutritional value (let’s say 100 calories each of sweet potato, tomato and kale), these would have individual ANDI values per calorie of 181, 186 and 1000 respectively. Add these together and you get 1367. Multiplying by 100 calories (the amount of each consumed) gives 136700. Divide this by 300 and you get a total ANDI score of 455.7.
Basically, the higher the score, the healthier the food.
What does ANDI measure?
ANDImeasures calcium; the carotenoids – beta carotene, alpha carotene, lutein, zeaxanthin, and lycopene; fibre; folate; glucosinolates; iron; magnesium; niacin; selenium; vitamins B1 (thiamine), B2 (riboflavin), B6, B12, C, and E; and zinc, plus the ORAC (oxygen radical absorbance capacity) score X 2. Most importantly, the ANDI scores are based on calories, not volume or weight of food, so a lower-calorie food with more nutrients scores higher than a calorie-dense food, which is why foods like iceberg lettuce and kale score high.
Have a look below and see how popular foods stack up in terms of micronutrient density per calorie. The more nutrient-dense food you consume, the more you will be satisfied with fewer calories.
So can diet really reverse diseases? And if so which diseases?
The following are some testimonials from Dr. Fuhrman’s patients. (Full TED Talk video covering the issues in this blog can be viewed below.)
[su_box title=”HIPPOCRATES” style=”glass” box_color=”#9cea59″ title_color=”#fbe42b” radius=”10″]Let food by thy medicine and let medicine be thy food.[/su_box]
G-BOMBS
Dr. Fuhrman coined the acronym G-BOMBS (Green Beans Onions Mushrooms Berries & Seeds) to represent those foods he considers are the immune system’s “special forces” – inhibiting fat storage, preventing cancer and prolonging our healthy lifespan.
I hope you are able to use this information to enjoy a diet that has food fighting for you rather than against you. After all, we are the food we eat – quite literally…
TED Talk Video
About Dr. Fuhrman
Joel Fuhrman, M.D. is a board-certified family physician, six-time New York Times best-selling author and internationally recognised expert on nutrition and natural healing.
He specialises in preventing and reversing disease through nutritional methods. He coined the term “Nutritarian” to describe his eating style, which is built around a diet of nutrient-dense, plant-rich foods.
For over 25 years, Dr. Fuhrman has shown that it is possible to achieve sustainable weight loss and reverse heart disease, diabetes and many other illnesses using smart nutrition. In his medical practice, and through his books and television specials, he continues to bring this life-saving message to hundreds of thousands of people around the world.
Dr. Fuhrman is the President of the Nutritional Research Foundation. He is also a member of the Dr. Oz Show Medical Advisory Board. He is a graduate of the University of Pennsylvania (Pearlman) School of Medicine (1988) and has received the St. Joseph’s Family Practice Resident’s Teaching Award for his contribution to the education of residents.
References
Dr. Fuhrman’s TED Talk (from which slides were taken)
Researchers at Stanford University School of Medicine just published results from a 12-month study which aimed to identify which diet was the best – Low-carb or Low-fat. And the winner is…
Well, first, let’s see what were the basic questions (hypotheses) that the leader researcher, Professor Christopher Gardner and his team were aiming to answer whether either of the following factors would dictate your success at losing weight:
Genotype (that which predicts other factors such as your eye colour), or
Baseline insulin secretion level (how much insulin your body produces to process glucose).
And the winner was?
Neither.
No evidence was found for the existence of a genotype or a baseline insulin level that would clearly favour your chances of losing weight.
Both diets resulted in an overall weight loss:
An average 13 pounds / 5.8 kg weight loss within the 609 study subjects
Wide variability – some gained as much as 20 pounds/9 kg while others lost as much as 60 pounds / 27 kg.
More detail about the methodology used can be found here.
Conclusions from the Research
Professor Gardner says “We have all heard stories of a friend who went on one diet – it worked great – and then another friend tried the same diet, and it didn’t work at all. It is because we are all very different, and we are just starting to understand the reasons for this diversity. Maybe we should not be asking what is the best diet, but what is the best diet for whom?”
His takeaway lesson from this study was that we should eat:
less sugar,
less refined flour,
more wholefoods (e.g. “wheatberry salad or grass-fed beef “), and
as many vegetables as possible.
Future projects are likely to focus on questions related to:
the microbiome (the billions of bacteria in our guts),
epigenetics (looking at gene expression rather than potential changes to the genetic code itself)
He goes on to say “I’m hoping that we can come up with signatures of sorts…I feel like we owe it to Americans to be smarter than to just say ‘eat less.’ I still think there is an opportunity to discover some personalisation to it.”
In his own words:
What Others Say
In the Telegraph article that discussed this research, they drew the conclusion that “the research showed the key to losing weight was simply eating less.”
Tam Fry, from the National Obesity Forum, a UK campaign group, said: “The best diet in town is not a fad but much less of what you actually fancy – and stick to it.”
Some Thoughts
The findings of the research do not surprise me at all. And I applaud some of the conclusions that Professor Gardner draws – cutting down on (refined) sugars/flours, eating more (plant) wholefoods and vegetables – but there are some issues that require clarification.
When weight loss is the only factor considered, other issues related to the overall health-promoting aspects of nutrition are marginalised. There appears to be no stated justification for Professor Gardner’s jump from talking about the results of the research (genotype and insulin secretion levels) to then recommending specific nutritional elements (less sugar, more wholefoods etc). If he is going to make these statements (especially if he includes “grass-fed beef” in the list of healthy wholefoods), then it would be useful to see some justification for such statements – and, as we would suspect, any justification would not come from a study that simply focuses on weight-loss without also measuring other health factors (cholesterol, triglycerides, mineral/vitamin balance, etc).
Professor Gardner’s statement “It is because we are all very different, and we are just starting to understand the reasons for this diversity. Maybe we should not be asking what is the best diet, but what is the best diet for whom?” is somewhat misleading. It suggests that there is no evidence from large population studies (such as the largest of them all, The China Study) that optimal health appears to depend on diet, to a large extent, irrespective of the individual genetic variations within the members of that population. Indeed, the Stanford University research itself dismisses the primacy of genetics or “insulin secretion levels” as markers for future weight gain, let alone the uncharted, and more vital area, of overall health gain.
There appears to be a misunderstanding in the media about what conclusions can be drawn from the study. Professor Gardner says “I feel like we owe it to Americans to be smarter than to just say ‘eat less.’ The Telegraph, on the other hand, states that “the research showed the key to losing weight was simply eating less.” No wonder the public get confused. And to add more confusion, Tam Fry (National Obesity Forum) states “The best diet in town is not a fad but much less of what you actually fancy – and stick to it.” Again, the implicit assumption here is that all foods are equal, all diets that do not include “moderation in all things” are fad diets, and, again, the mistaken implication that the research is suggesting we should simply eat less calories.
Professor Gardner’s comment “Maybe we should not be asking what is the best diet, but what is the best diet for whom?” is, for me, a frankly shocking indication that he may not have looked at the wealth of research demonstrating that there is one diet that has been proven to be optimal for human health – a whole food plant-based diet, with minimal or no animal protein. I suspect that if his research subjects had been rural Chinese, Papua Highlanders, Central Africans or Tarahumara Indians from northern Mexico, then he would not have even bothered to do this research study since more or less everyone within those communities would already have been at their optimal body weight, largely regardless of genome or insulin secretion level.
When such research projects are taken up by the media and then the public, they are thrown back, once again, on the mistaken belief that nutrition is simply a matter of the quantity and not quality of the calories being “eaten”. People do not eat calories. They eat food. And our bodies are made out of the food we eat.
Yet again, this research focuses in a reductionist manner on genetic and individual biochemical responses in order to establish something so vitally important to our populations’ health and well-being. It still makes me recall Nero fiddling while Rome burned…
In my experience and that of my clients, even increasing the amount of calories consumed after making the transition to a WFPBD (whole food plant-based diet) from a standard diet (whether it be a meat-based, vegetarian or vegan diet), can cause excess fat to drop off the body. Just as a vitamin C supplement does not cause the same bodily responses as compared to the vitamin C derived from eating an apple, the calories “consumed” from eating animal foods (whether processed or unprocessed) have a very different effect on the body than those derived from eating plant foods (whether organic whole plants or even less-healthy processed plant-foods). And the added bonus from eating a wide variety of organic whole plants represents yet another step in the direction of optimal health from eating those less-healthy processed plant foods.
Gardner CD, Trepanowski JF, Del Gobbo LC, Hauser ME, Rigdon J, Ioannidis JPA, Desai M, King AC. AMA. 2018 Feb 20;319(7):667-679. doi: 10.1001/jama.2018.0245. Effect of Low-Fat vs Low-Carbohydrate Diet on 12-Month Weight Loss in Overweight Adults and the Association With Genotype Pattern or Insulin Secretion: The DIETFITS Randomized Clinical Trial.
We are constantly bombarded by new claims about the benefits of taking this or that supplement. The implicit assumption made by this emphasis on supplementation is that a varied and healthy diet alone can’t supply everything that the body needs to maintain homeostasis – that is, its optimal natural balance. I want to challenge this assumption and put whole plant foods back at the top of the Must Have list…
First, let me introduce you to someone I expect many of you have never even heard of – Dr Rui Hau Liu, PhD, MD (see bottom of post for more information about his academic and professional qualifications).
Dr Liu makes it makes it clear that the majority of all the current and past scientific evidence suggests that it is the whole plant food approach, and not the dietary supplement approach, that is the powerful solution for cancer prevention and health promotion. He points out that a dietary supplement (which might contain one compound or multiple compounds) “… cannot mimic a natural combination of the bioactive compound in foods, vegetables, and whole grains.” And the scientific literature suggests that “…the single antioxidant, single bioactive compound approach is not working. For example, beta carotene, selenium, vitamin E and vitamin C alone to prevent cancer is not as effective as a combination of the compound from the whole fruit.” (From a lecture in Diseases of Affluence module 2.16 of the eCornell Certificate in Plant Based Nutrition.)
His advice is that, instead of trusting expensive dietary supplements, we should eat a wide variety of fruits, vegetables, whole grains and other plant-based foods – whether these be processed, raw, cooked, dried, fresh, canned, frozen or in the form of 100% whole plant juices. The important thing is to increase the plant-based portion sizes that we consume. Some bioactive compounds are more bioavailable without processing, and some others are more bioavailable after cooking. For instance, the antioxidant benefits of the lycopene in tomatoes increases after cooking.
Dr Liu looked at whole plant food consumption compared with supplements. His team increased the number of apples (from 1 to 6 apples per day) fed to study animals. While the supplements had little or no effect (and in some of his studies, injurious effects), apples both inhibited tumour appearance and caused existing tumours to grow more slowly. The thing here is that it is not an isolated component of the food item (in this case apple) that can be extracted and made to be useful; rather, it has to be a matter of taking nature’s “medicine” in whole natural form, so that our bodies can absorb and utilise the bioactive components.
This then permits all the hugely complex range of bioactive compounds to come into play – many, perhaps the vast majority of which, we do not yet even know. These include secondary metabolites and antioxidants such as the carotenoids, phenolic acids, and flavonoids and many other compounds.
To illustrate this, here are just a few of the known bioactive components within just six divisions of the flavanoid group:
There are many other flavonoids, including some of the more common ones called aurones, xanthones, and condensed tannins.
We have little idea yet about how the 8,000 or so known bioactive compounds in fruits, vegetables and whole grains relate to and depend upon each other. And, again, it is thought that there are many thousands more yet to be discovered. It is not, therefore, difficult to understand that food components and nutrients work synergistically in whole foods, through a complex variety of different mechanisms. We cannot replicate the benefits of food with isolated chemical supplements.
The complexity is simply mind-boggling and will probably always be beyond our minds to comprehend, and our scientific instruments to measure. However, we would be able to see the results in those individuals and populations whose habitual diets consist largely or exclusively of whole plant foods.
Evolutionary processes, over vast aeons of time, have equipped plants with intricate and highly effective defences against everything from damaging sunlight radiation and hungry insects, to fungi, viruses and bacteria. And, slowly but surely, evolution has also established mechanisms through which our human bodies are able to access and extract these bioactive plant compounds and, thus, take advantage of their beneficial properties.
So, the next time we are encouraged to buy the latest miracle dietary supplement, perhaps we’ll give it a miss – we get enough a mouthful of miracles every time we bite into a juicy apple.
Dr Rui Hau Liu, PhD, MD
Rui Hai Liu is a Professor in the Department of Food Science at Cornell University. He received his PhD in Toxicology from Cornell University in 1993. He also holds a MD in Medicine and a MS in Nutrition and Food Toxicology. Dr Liu was a Research Associate in the Department of Clinical Sciences in the College of Veterinary Medicine at Cornell University.
His research program focuses on diet and cancer, effect of functional foods/nutraceuticals on chronic disease risks, and bioactive compounds in natural products and herbal remedies for anticancer and antiviral activity.
His specific interests include:
1) health benefits of phytochemicals in fruits, vegetables, and whole grains;
2) food genomics and functional foods for disease prevention and health promotion targeted at cancers, aging, and inflammatory diseases; and
3) natural products and herbal formulations for antiviral activity to hepatitis B and C.
Thomson Reuters recognized Liu as one of the world’s most influential scientific minds for 2014 and 2015 and named him as a highly cited researcher.
He has published more than 145 scientific papers in peer-reviewed journals and accrued over 11,100 citations. Essential Science Indicators ranked him as one of the top five scientists in the field of agricultural sciences, including nutrition and food science. In 2011, he received the Institute of Food Technologists’ Babcock-Hart Award for outstanding contributions to the field of food science in the improvement of public health through nutrition.
Note: For more information on Dr. Rui Hai Liu’s work visit Cornell University.
References
Boyer J, Liu RH. Nutr J. 2004; 3(5). Apple phytochemicals and their health benefits.
Ali Ghasemzadeh. Neda Ghasemzadeh. Journal of Medicinal Plants Research Vol. 5(31), pp. 6697-6703, 23 December, 2011. Available online at http://www.academicjournals.org/JMPR. Flavonoids and phenolic acids: Role and biochemical activity in plants and human.
Campbell TC, Jacobson H. Benbella Books, Dallas TX. 2013. Whole: Rethinking the Science of Nutrition.
Eberhardt MV, Lee CY, Liu RH. Nature. 2000 Jun 22; 405(6789): 903-4. Antioxidant activity of fresh apples.
Liu RH, Liu J, Chen B. J Agric Food Chem. 2005; 53:2341-2343. Apples prevent mammary tumors in rats.
Science Watch Author Commentaries. (2012). http://archive.sciencewatch.com/inter/aut/2012/12-jan/12janLiu/. Rui Hai Liu on studying the health benefits of whole foods.
Dean Ornish et al. https://www.ornish.com/wp-content/uploads/8369.full_.pdf?4ae29f. Changes in prostate gene expression in men undergoing an intensive nutrition and lifestyle intervention.
Dean Ornish. https://www.ornish.com/wpcontent/uploads/Intensive_Lifestyle_Changes_and_Prostate_Cancer.pdf?4ae29f. Intensive Lifestyle Changes May Affect the Progression of Prostate Cancer.
David Palma, Tom Pickles. https://www.ornish.com/wp-content/uploads/telomerase-benefits-healthy-living1.pdf?4ae29f. Telomerase and the benefi ts of healthy living.
T Colin Campbell. https://nutritionstudies.org/mystique-of-protein-implications/. The Mystique of Protein and Its Implications.
Preventative Medicine Research Institute. http://www.pmri.org/
Video recorded at UR Nutrition in Medicine’s Lunch with Docs on April 8th, 2017. Nutrition and Cancer, Lecture from Dr. Thomas Campbell
There are so many diets out there – drinking dirty bathwater, swallowing tapeworms and inserting yogurt enemas – each claiming its own miracle cure for weight worries and disease distress. But does this display a genuine concern for one’s health?
Most people try and fail at some kind of New Year’s resolution, and most of these are connected to ways in which we want to improve our health – generally diet or exercise. Wreckage of our best intentions are visible in a garage or spare bedroom full of dumbbells, overpriced running trainers, and cross-training machines.
This concern about weight and diet is nothing new:
In 1087, William the Conqueror was already morbidly obese and decided to fight his own battle of the bulge with an alcohol-only diet. Big Bill took to his bed and refused everything but liquids until he had shed the pounds. Ironically, this didn’t really do him any health favours as later that year, when he’d lost enough weight to get back on his horse, he was thrown from his trusty steed, ruptured his gut, and died in agony. He was still so large, his body had to be wedged into the stone coffin.
In 1760, Dr Flemyng’s soap diet recommended eating soap to shed the pounds. Flemyng reasoned that as soap removed fats and oils from clothes it could also wash away excess fat from inside the body. His patients were told to eat soap made from alkaline salt, oil and fat dissolved in quicklime and water. When soap diet devotees complained that they were just as fat as they were when they started the diet (though hopefully somewhat cleaner), he insisted they must be eating the wrong soap or in the wrong amount.
In the 18th century, the Bath water diet attracted thousands to spa towns in order to ‘take the waters’. And this was not just bathing in the mineral-rich baths, it also involved quaffing back gallons of unfiltered water that hundreds of other people have sweated and stewed themselves in each day.
In 1810, the Vinegar Diet of British surgeon William Wadd (1776-1829) was published in his ‘Cursory Remarks on Corpulence’. Drinking large quantities of vinegar would supposedly dissolve fat. The poet Lord Byron (1788-1824) was an advocate of this particular diet plan as he was morbidly fixated with his weight and had yoyo dieted all his life. Records show in 1806 he weighed 13st 12lb (88kg), but by 1811 Byron weighed under 9st (57kg). In order to purge his body and melt away fat, not only would Byron drink vinegar each day, but he restricted solid foods to potatoes – soaked in vinegar. And the vinegar diet still does the rounds of the “out there” diets to this day.
In 1863, the first low-carbohydrate diet book ‘Letter on Corpulence, Addressed to the Public’ was written by William Banting. Meat for breakfast, lunch and dinner. The original Banting diet forbade complex carbohydrates, beer, starchy fruit and veg and dairy, but lean protein, eggs, and the odd sherry with a claret chaser were fine.
At the start of the the 20th century, John Harvey Kellogg (1852-1943), of cornflake fame, manufactured plain cereals to suppress sexual urges. The so-called “masturbation diet” not only promised to improve health, aid digestion and regulate weight, but it would also stop you masturbating. Kellogg (and many other doctors) argued that masturbation caused ‘cancer of the womb, urinary diseases, nocturnal emissions, impotence, epilepsy, insanity, and mental and physical debility’. He reasoned that spicy, ‘exciting’ food, overly stimulated the senses, therefore the plainer your diet the less inclined you would be to give yourself a treat. Yoghurt enemas were also encouraged by Kellogg, who actually invented a machine to administer such enemas to his patients. The latter dietary innovation never really caught on the way cornflakes did.
In the late 19th century, Horace Fletcher was a great proponent of the mastication diet where you were required to chew each mouthful of food 100 times. The theory was that the food would become liquefied, which meant the chewer wouldn’t overeat and the mush would be easier to digest. Fletcher claimed his method of eating produced stools “with no stench, no evidence of putrid bacterial decomposition, only with the odour of warm earth or a hot biscuit”. Apparently, Fletcher carried around a sample of his own faeces to back up this claim should anyone challenge him on this point. He became known as ‘the Great Masticator’, although I imagine there were variations of this nickname.
In the 1920’s, ‘obesity soaps’ were produced by companies in London. This more recent version of s soap diet ony promised that internal fat would dissolve if people washed with i. Luckily, eating it was not necessary this time round.
And there are many, many more diets throughout history which have tried to help with a seemingly insatiable public appetite for weight-reduction and improved health through dietary interventions – smoking yourself to thinness, taking vast quantities of speed, dosing up on sugar, using radium, eating nothing but cabbage, fish, milk or eggs – even taking arsenic to shed those extra pounds.
We can all laugh at historical diets, but there are few signs in the 21st century of a slowing-down in similar attempts to achieve optimal weight and health (with minimal effort). The internet is awash with dodgy diet pills and pseudo-scientific weight loss advice (tried the zodiac diet lately?).
It appears that if a media-reported “scientific study” told us that by drinking a bottle of grimy, slightly hairy bathwater we would definitely lose weight, some people would actually try it – you know they would! I mean, Beyoncé once advised us to eat nothing other than maple syrup and Reese Witherspoon advocated eating a diet consisting solely of baby food.
This obsession with diet can be viewed as an indication of a fundamental human desire to be healthy.
I can get annoyed at how so many companies and individuals make profits out of peddling diets that will eventually fail; but it makes me sad that the only thing people need to do in order to achieve optimal health and ideal body weight is to eat what all the healthiest human populations have always eaten – a diet largely or completely consisting of whole plant foods.
Sometimes the most obvious solution can be the most difficult to swallow…
Our bodies are creating thousands of microscopic cancer cells all the time. Whether these “cancers without disease” are fed by new blood vessels depends more on our diet than we realise.
When the body is working properly, cancer cells don’t get sufficient blood supply to grow. This is one of our most important defences against the exponential growth rate of cancers. When angiogenesis is “turned on”, and the cancer cells are fed by sufficient blood vessels, tumours can develop. Antiangiogenic therapy aims to starve the cancer of its blood supply, thus rendering the isolated cancer cells harmless.
If you took all the blood vessels in your body and laid them end to end, they would be around 60,000 miles in length and could encircle the Earth twice.
So what has this to do with diet?
Dr William W Li, an internationally acclaimed expert in angiogenesis and diet considers that food is a powerful, yet largely untapped resource that can prevent, halt and even reverse life-threatening chronic diseases. He believes that:
more than 80 percent of heart disease, stroke, obesity and type 2 diabetes cases are preventable by dietary changes
around 40 percent of all cancers are preventable by diet changes
The Angiogenesis Foundation has discovered and gathered evidence that fruits, vegetables, herbs, seafood, tea, coffee, and even chocolate contain natural substances — bioactives — that can prevent and intercept disease by influencing angiogenesis and other defence systems in the body.
“What we eat and drink is enormously impactful when it comes to preventing disease.” *
In addition to the food itself, Dr Li considers the specific cultivated variety, processing and cooking methods and even food combinations also play a significant role in how diet will affect disease progression.
“Using the same research systems and methodologies we use to test medicines, we test varieties and combinations of foods, beverages, and ingredients and how cooking, processing, and storage impact their potency against disease. We discover how to eat foods, drink beverages, and utilize ingredients with the most prevention activity to optimize their effects. Our vision is food will be the ultimate delivery vehicle for natural bioactive molecules that prevent diseases in their earliest stages.” *
Some foods being researched for their antiangiogenic properties
He has demonstrated that various foods can turn off the blood supply to tumours. And, because not all foods have the same bioactive properties, the aim is to identify which specific varieties of food are best.
This will then provide us with a choice – do we have a standard cup of builder’s tea in the morning, or do we have a type of tea that has been shown to have the highest levels of disease-inhibiting (i.e. in this context, antiangiogenic) properties?
Some teas (in combination) are more antiangiogenic than others.
And this information is not merely anecdotal opinion of the type we hear every day expressed in the media; this is scientifically validated data that people can use to make informed decisions about the foods they eat, and how those foods are likely to improve their defences against life-threatening chronic diseases.
This may be an area that you have not thought about a great deal. It is common knowledge these days that blood vessels can be damaged by eating certain foods (largely animal-based, processed foods high in fat, salt and sugar). The endothelial cells that line the inside of blood vessels can become hardened, narrowed, furred-up, blocked with jagged plaques and then catastrophically fail on us – resulting in life-threatening events. But the idea that blood vessels can be repaired, re-grow and that new blood vessels can form – these are not so much thought about. It is easy to see it happening when you, for instance, cut your hand. Blood vessels are damaged, clots form, new blood vessels repopulate the area of the clot and your skin is restored to is former state.
However, when clusters of cancer cells attract the creation of new blood vessels to provide them with the oxygen and nutrients required for growth, we have a wonderful biological phenomenon which is, sadly, able to undermine our body’s health.
The research that Dr Li and his colleagues are undertaking derives from extensive experience in the field of pharmaceutical health interventions. This background allows him and his researchers to compare the effects of pharmaceuticals (some of which they are responsible for testing and developing) with the effects of food.
In the table shown here on the left, the blue and green bars are cancer and common drugs. Their effectiveness is indicated by how far they extend to the right (i.e. how antiangiogenic they are). The red bars are dietary factors (common foods, such as garlic and green tea).
You will notice that in most cases the dietary factors are as effective or even more effective than the drugs. If this doesn’t cause us to pause and reflect on the massive implications that this has for our societies, then what will?
Naturally, there is no profit for the Toxic Triad (Big Pharma, Big Farming and Big Food) from populations maintaining their health by eating and drinking well. And these powerful industries spend £billions on legal battles, government/institutional funding and blanket advertising. They do not want the public to know that food can be our best medicine.
A fine example of the research that can help us to appreciate the value of dietary intervention, is the study undertaken by the Harvard School of Public Health which found that the risk of developing prostate cancer in men was significantly reduced by simply eating more tomatoes in their regular diet.
Perhaps we will know that something is starting to change for the better when we see insurance companies reducing their clients’ premiums if they can prove that they are eating a healthy diet. They already ask questions about smoking habits, involvement in risky sports or professions, and whether or not the potential client has had any illnesses that might be relevant to a life insurance claim.
There are obviously some moves in this direction starting to happen…
I would recommend that you watch Dr Li’s short TED talk (see below). If you want to know more about this fascinating area of research, please look here or contact me and I will expand further on the topic.
William W. Li is Chief Executive Officer, President, Medical Director, and Co-founder of the Angiogenesis Foundation. Trained in the lab of Dr. Judah Folkman, pioneer of the angiogenesis field, Dr. Li has been actively engaged in angiogenesis research and clinical development for 30 years. Under his leadership, the Foundation has developed a unique social enterprise model based on value creating collaborations with leading medical academic centres, biopharmaceutical and medical device companies, and government agencies, including the National Institutes of Health, Food and Drug Administration, and centres for Medicare and Medicaid Services.
As President, Dr. Li has testified and presented before congressional and other government panels on the impact of angiogenesis in healthcare, and lectures around the world on angiogenesis-related topics in front of clinical, government, and industrial audiences. He is actively engaged in global efforts to advance the applications of angiogenesis-based therapeutics across diverse medical fields, including oncology/haematology, cardiology, ophthalmology, vascular surgery, dermatology, wound care, and regenerative medicine. He has been published in Science, The New England Journal of Medicine, The Lancet, Nature Reviews and other leading peer-reviewed medical journals.
Dr. Li received his A.B. with honours from Harvard College, and his M.D. from the University of Pittsburgh School of Medicine. He completed his internship, residency, and fellowship training in General Internal Medicine at the Massachusetts General Hospital in Boston. He has held appointments on the clinical faculties of Harvard Medical School, Tufts University School of Veterinary Medicine, and Dartmouth Medical School. He serves as adviser and consultant to leading global public and private companies.
References
Judah Folkman & Raghu Kalluri. Nature 427, 787 (26 February 2004) doi:10.1038/427787a. Cancer without disease.
Rebecca E Graff, Andreas Pettersson, Rosina T Lis, Thomas U Ahearn, Sarah C Markt, Kathryn M Wilson, Jennifer R Rider, Michelangelo Fiorentino, Stephen Finn, Stacey A Kenfield, Massimo Loda, Edward L Giovannucci, Bernard Rosner, and Lorelei A Mucci. Am J Clin Nutr. 2016 Mar; 103(3): 851–860. Published online 2016 Jan 27. doi: 10.3945/ajcn.115.118703. PMCID: PMC4763492. Dietary lycopene intake and risk of prostate cancer defined by ERG protein expression.
Li WW, Li VW, Hutnik M, Chiou AS. J Oncol. 2012; 2012: 1-23. Tumor angiogenesis as a target for dietary cancer prevention.
The 1958 Delaney Amendment stated that “…no additive is deemed safe if it is found [in “appropriate” tests] to induce cancer when ingested by man or animal…” This US amendment required zero tolerance – that is, no amount of any substance found to be carcinogenic could be added to food. Of course, we know that this noble goal was never achieved and now we have carcinogenic food additives and carcinogenic food processing methods.
£billions are spent researching potential carcinogens found in the environment rather than those found in food. Why is this? Simply, it is easier to get funding for this type of reductionist research than it is to deal with the complexities of human nutrition on a population-wide basis. Also, the so-called Toxic Triad of Big Food, Big Farming and Big Pharma put political and commercial pressure (and lots of it) on research institutions to avoid pointing the finger at powerful food manufacturers, distributors and sellers who make huge profits and contribute huge sums to both government and academic institutions around the world.
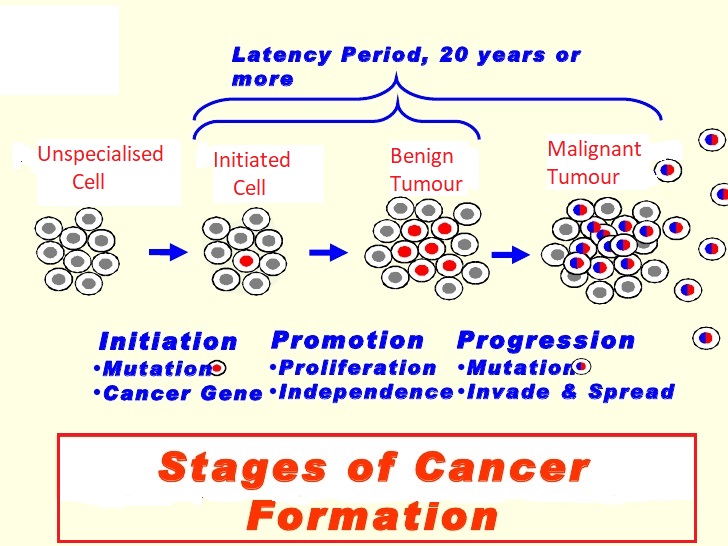
The three phases of cancer
Also, there has been an overwhelming emphasis on the first phase of the three phases of cancer (Initiation, Promotion & Progression).
Genetic science appears to be somewhat hamstrung by a particular paradigm. Within this paradigm, consideration is almost solely given to the concept that the only approach we can take is to try and prevent cancers by avoiding the Initiation stage (which happens in a tiny fraction of a second) when DNA is first exposed to carcinogens at the point of cellular reproduction. Once the cancer has passed to the Promotion (years to decades) or Progression (usually years) stages, the seemingly unchallenged consensus appears to be that there is no point in doing anything other than turn to one of the three ugly sisters – surgery, radiation or chemotherapy. As we will see later, there is strong evidence that cancer can be slowed, halted and even reversed completely throughout the Promotion stage and, to perhaps a lesser degree, in the Progression stage of cancer development.
Much of the focus of scientific research, government legislation and media coverage is on individual non-dietary carcinogens (such as radon or asbestos). And even when researchers do deal with diet-related carcinogens, the emphasis for most part is on those carcinogens that are unintentionally included in the food cycle (such as aflatoxin in corn and peanut mould or 2,3,7,8-Tetrachlorodibenzodioxin which is produced during the manufacture of chlorinated hydrocarbons). This tendency can be seen, for instance, in this quote from a section entitled Types of Food Contaminants (my bold highlighted text) in a peer-reviewed paper entitled “Carcinogenic Food Contaminants”:
“There are four primary types of potentially carcinogenic compounds that have been examined to determine if they act as carcinogens in humans. The first are natural products that may be present in food and are unavoidable. For example, the process of creating salted fish produces carcinogens which can not be easily avoided. Second, are natural products that might be avoided such as the contamination of grain with the carcinogenic fungal metabolite aflatoxin, which can be reduced or eliminated using best practices for grain storage. Third, anthropogenic chemicals may be present in food. For instance, 2,3,7,8-tetracholordibenzo-p-dioxin has been inadvertently produced during the manufacture of chlorinated hydrocarbons, but it contaminates the environment, resists degradation, and accumulates in certain foodstuffs. A fourth category of concern is anthropogenic chemicals intentionally added to foods, such as saccharin or food coloring, but these are not addressed in this review because they are not contaminants because they are added intentionally.”
It may be an erroneous assumption, but could this stated avoidance of investigating those dietary carcinogens “intentionally” added to our food be motivated by hidden political/commercial pressures to do so? The paper continues (my bold highlighted text) to this conclusion:
“The accumulation of evidence sufficient to render judgement on food contaminants and human cancer risk is a daunting task…several food contaminants have been confirmed as carcinogenic to humans. Possibly the clearest example is the finding that aflatoxin is a major cause of liver cancer…”
Again, we see a tendency to seek the “clearest” (read “easiest to research”) examples of dietary carcinogens as well as a tendency to miss the elephant in the room – namely, the fact that ALL cancers and other diet-related chronic diseases (e.g. heart disease, diabetes, obesity) are rising around the world at a pace perfectly in parallel with the equal rise in adoption of the Standard American Diet (SAD).
There are reported to be between 80,000 and 100,000 environmental chemicals that would need to be thoroughly tested in order to establish whether or not they each represent a significant cancer risk for humans. Imagine how long that would take? As research teams trawl through these, the focus on the avoidable (i.e. both those intentionally avoided “intentionally added”) dietary carcinogens referred to above would continue to be unwittingly consumed by millions of people. And this is aside from those carcinogens that are not added to foods, but actually ARE the foods, such as our next and main topic casein in dairy.
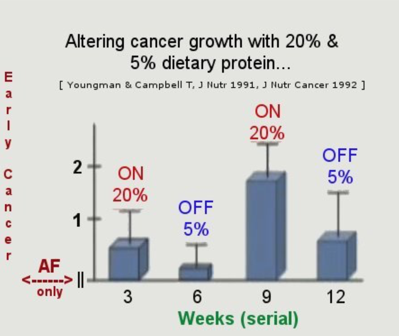
The animal protein used by Professor T Colin Campbell and his team of researchers was casein, which represents around 85% of all the protein in cow’s milk. He demonstrated that you could turn cancer tumours on and off in rats and mice merely by alternating the amount of protein consumed from 5% to 20% and then from 20% back down to 5% of their total daily calorie intake. Since this research, which is now decades old, he was able to identify the precise mechanisms concerned and how they are involved in all three phases of cancer development.
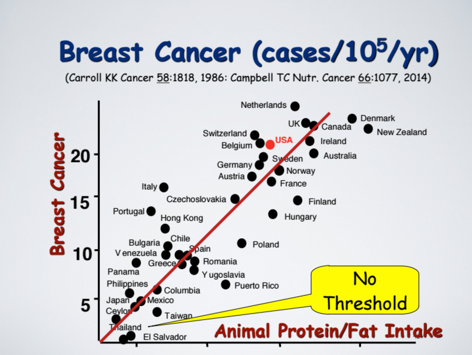
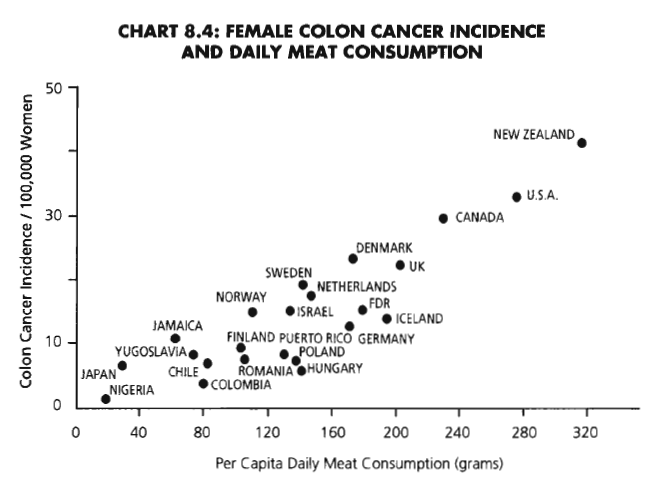
He is also convinced that other animal proteins have the same detrimental effects – that is, if animal protein intake is increased then cancer risk also increases; but if animal protein intake is reduced then the cancer risk decreases. This can be witnessed in human populations. The following graph shows the example of breast cancer and its geographical spread by country and quantity of average national levels of animal protein (and in this case, also animal fat) consumption. The USA is highlighted in red, but the UK has even higher incidence of breast cancer per capita, reflecting the corresponding higher protein (and fat) intake.
The following chart from The China Study shows female colon cancer rising with meat consumption.
And just to hammer home the correlation between animal protein consumption and incidence of cancer, I have included these further charts from other research:
Assuming a causal rather than a merely correlational relationship between these factors, we can identify the particular protein’s amino acid composition as the specific reason for the adverse effects. Sufficient studies for more than 50 years have shown that the nutritional responses of different proteins are attributed to their differing amino acid compositions; and the differences in nutritional response between animal and plant proteins disappear when any limiting amino acids are restored. Limiting amino acids are those essential amino acids which are present in only small quantities within any given food. The only “food” completely lacking one essential amino acid is gelatin which completely lacks tryptophan. All other foods, as far as I am aware, contain all the essential amino acids, but – and this is the significant point – in varying amounts.
Throughout many experiments over a period of over 30 years, Professor Campbell’s research team found that casein in particular was a powerful promoter of cancer, with two of the major contributory factors being:
increased production of growth hormones, and
elevated body acid load (metabolic acidosis).
Unlike animal proteins such as casein, plant proteins (for instance, the protein in wheat) does not stimulate cancer development. However, as indicated above – when wheat’s limiting amino acid, lysine, is restored to the relevant level, wheat protein acts just the same as casein in terms of cancer promotion.
So, to recap:
animal and plant proteins are not the same
the variation is due to their different amino acid compositions
these different amino acid compositions produce different nutritional responses.
While animal proteins do vary between themselves, any difference is much less than the degree to which they differ from plant proteins as a whole, and there is virtually no overlap between the two groups of protein.
The conventional way in which the so-called “quality” or “completeness” of a protein is determined relates to protein’s efficiency ratio. Thus, plant proteins are described as having LBV (Low Biological Value) while animal proteins are HBV (High Biological Value) depending on how many grams of gain in body weight occur with a given intake of the protein:
Animal proteins cause a greater weight gain over a specified period of time
Plant proteins cause a lesser weight gain over a specified period of time.
Thus,
Egg, meat, cow’s milk, and fish promote a faster rate of growth
Rice, beans and wheat flour promote a slower rate of gain.
So what’s wrong with that?
Nothing, if you want your farm animals to grow rapidly to return the maximum profit over the shortest time; but not if you are a human. Rapid growth in childhood is not a beneficial thing and rapid growth of cancer cells in childhood or adulthood is generally accepted as undesirable.
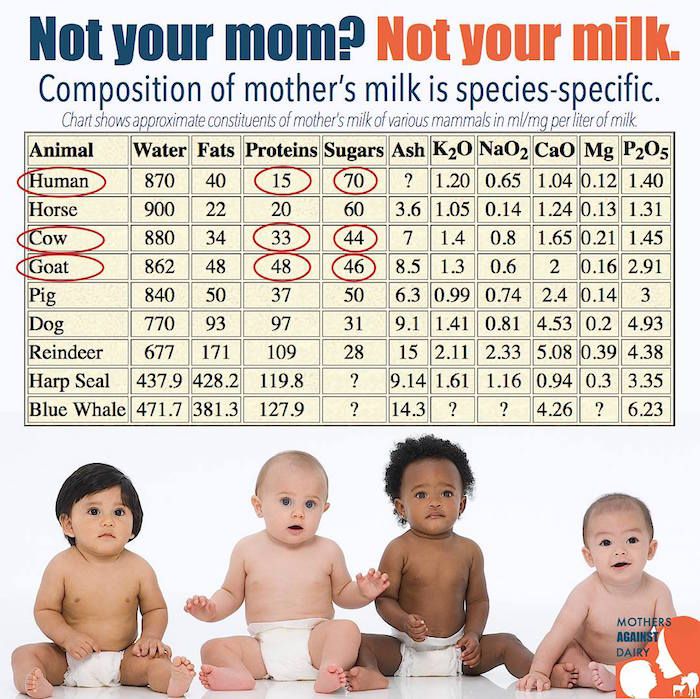
Cow’s Milk is Baby Calf Growth Fluid
And, as Dr Michael Klaper says: “The purpose of cow’s milk is to turn a 65-pound calf into a 700-pound cow as rapidly as possible. Cow’s milk IS baby calf growth fluid. No matter what you do to it, that is what the stuff is.”
It appears at first sight to be a truly shocking that Professor Campbell should define casein in dairy as “The most relevant cancer promoter ever discovered.”
But it is possible to understand this when one considers the increasingly ubiquitous role that dairy plays in the majority of diets. Dairy products are in everything from pizzas to puddings, sherbets to soups. I needn’t tell you how much the dairy industry promotes its supposed (and largely discredited) health benefits – you just need to turn on the TV or flick through a magazine. And the public at large are so taken in by the claims that it is good for your bones (debatable) and or that it is a health food (debatable).
Dr Neil Barnard from the PCRM (Physicians Committee for Responsible Medicine) goes just as far as Professor Campbell and Dr Michael Klaper. He says “Thanks to these marketing campaigns, milk myths abound in our culture. But science doesn’t support them.” Calling them “white lies” he goes on to attack the myths that the milk industry continues to promote to the public. (Click picture below to read his article, “White Lies? Five Milk Myths Debunked”.)
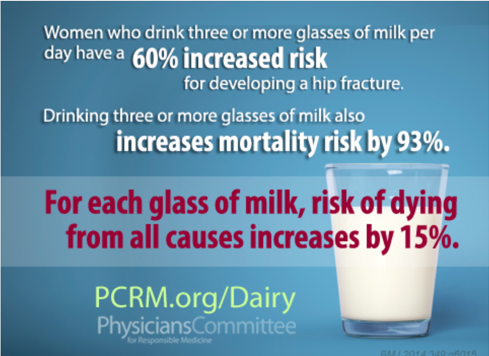
It occurred to me that one of the reasons that the dairy industry peddles the unsubstantiated myth about milk’s bone-building features is that it is a useful distraction from the potentially catastrophic impact of casein. Maybe I’m just being cynical…In any case, here’s Dr Michael Greger’s view on milk and bone health:
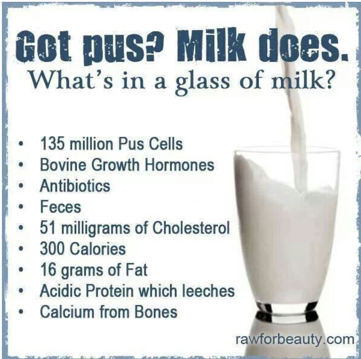
Finally, if you are still in doubt about whether or not people are wise to pour a bit of the white (or red) stuff into their breakfast cereal, I will leave you with a couple of self-explanatory posters about a rather distasteful ingredient that you won’t hear the dairy industry mooing about…
References
T. Colin Campbell. J Nat Sci. Author manuscript; available in PMC 2017 Oct 18. Published in final edited form as: J Nat Sci. 2017 Oct; 3(10): e448. Cancer Prevention and Treatment by Wholistic Nutrition.
David O. Carpenter M.D., Sheila Bushkin-Bedient M.D. Journal of Adolescent Health. Volume 52, Issue 5, Supplement, May 2013, Pages S21-S29. Exposure to Chemicals and Radiation During Childhood and Risk for Cancer Later in Life.
Campbell TC. J Nat Sci. 2017 Oct;3(10). pii: e448. Cancer Prevention and Treatment by Wholistic Nutrition.
Campbell TC. Nutr Cancer. 2017 Aug-Sep;69(6):962-968. doi: 10.1080/01635581.2017.1339094. Epub 2017 Jul 25. Nutrition and Cancer: An Historical Perspective.-The Past, Present, and Future of Nutrition and Cancer. Part 2. Misunderstanding and Ignoring Nutrition.
Campbell TC. Nutr Cancer. 2017 Jul;69(5):811-817. doi: 10.1080/01635581.2017.1317823. Epub 2017 Jun 8. The Past, Present, and Future of Nutrition and Cancer: Part 1-Was A Nutritional Association Acknowledged a Century Ago?
Campbell TM, Campbell TC. Isr Med Assoc J. 2008 Oct;10(10):730-2. The benefits of integrating nutrition into clinical medicine.
Sarter B, Campbell TC, Fuhrman J. Altern Ther Health Med. 2008 May-Jun;14(3):48-53. Effect of a high nutrient density diet on long-term weight loss: a retrospective chart review.
Campbell TC. MedGenMed. 2007;9(3):57. Fail to test the impressive ability of diet to favorably affect long-term health and body weight loss.
Campbell TC. Am J Clin Nutr. 2007 Jun;85(6):1667. Dietary protein, growth factors, and cancer.
Wang Y, Crawford MA, Chen J, Li J, Ghebremeskel K, Campbell TC, Fan W, Parker R, Leyton J. Comp Biochem Physiol A Mol Integr Physiol. 2003 Sep;136(1):127-40. Fish consumption, blood docosahexaenoic acid and chronic diseases in Chinese rural populations.
Feskanich D, Bischoff-Ferrari HA, Frazier AL, Willett WC. JAMA Pediatr. 2014 Jan;168(1):54-60. doi: 10.1001/jamapediatrics.2013.3821. Milk consumption during teenage years and risk of hip fractures in older adults.
Sun Z, Zhang Z, Wang X, Cade R, Elmir Z, Fregly M. Peptides. 2003 Jun;24(6):937-43. Relation of beta-casomorphin to apnea in sudden infant death syndrome.
Fiedorowicz E, Jarmołowska B, Iwan M, Kostyra E, Obuchowicz R, Obuchowicz M. Peptides. 2011 Apr;32(4):707-12. The influence of μ-opioid receptor agonist and antagonist peptides on peripheral blood mononuclear cells (PBMCs).
Kost NV, Sokolov OY, Kurasova OB, Dmitriev AD, Tarakanova JN, Gabaeva MV, Zolotarev YA, Dadayan AK, Grachev SA, Korneeva EV, Mikheeva IG, Zozulya AA. Peptides. 2009 Oct;30(10):1854-60. Beta-casomorphins-7 in infants on different type of feeding and different levels of psychomotor development.
A S Wiley. Biol. 2012 Mar-Apr;24(2):130-8. Cow milk consumption, insulin-like growth factor-I, and human biology: a life history approach. Am J Hum
B C Melnik, S M John, G Schmitz. Nutr J. 2013; 12: 103. Milk is not just food but most likely a genetic transfection system activating mTORC1 signaling for postnatal growth.
C Melnik. J Obes. 2012;2012:197653. Excessive Leucine-mTORC1-Signalling of Cow Milk-Based Infant Formula: The Missing Link to Understand Early Childhood Obesity.
M S Kramer. J Pediatr. 1981 Jun;98(6):883-7. Do breast-feeding and delayed introduction of solid foods protect against subsequent obesity?
B C Melnik. World J Diabetes. 2012 Mar 15;3(3):38-53. Leucine signaling in the pathogenesis of type 2 diabetes and obesity.
A S Wiley. PLoS One. 2011 Feb 14;6(2):e14685. Milk intake and total dairy consumption: associations with early menarche in NHANES 1999-2004.
D S Ludwig, W C Willett. JAMA Pediatr. 2013 Sep;167(9):788-9. Three daily servings of reduced-fat milk: an evidence-based recommendation?
K Arnberg, C Molgaard, K F Michaelsen, S M Jensen, E Trolle, A Larnkjaer. J Nutr. 2012 Dec;142(12):2083-90. Skim milk, whey, and casein increase body weight and whey and casein increase the plasma C-peptide concentration in overweight adolescents.
P Wilde, E Morgan, J Roberts, A Schpok, T Wilson. Physiol Behav. 2012 Aug 20;107(1):172-5. Relationship between funding sources and outcomes of obesity-related research.
Youngman LD, Campbell TC. J Nutr. 1991 Sep;121(9):1454-61. High protein intake promotes the growth of hepatic preneoplastic foci in Fischer #344 rats: evidence that early remodeled foci retain the potential for future growth.
One of my clients emailed me to say that he was concerned about his blood pressure. On the WFPB programme for nearly four weeks, his blood pressure has been dropping consistently from around 160/100 when he started, to 113/78 two days ago. Then it looked like it was starting to rise again. I sensed some panic in his tone…
When I looked at his nutritional/lifestyle diary for the past days I could see the problem – sleep or rather the lack of it.
A recent study of US citizens found that 1 in 3 were chronically sleep deprived. It is likely figures for other Western countries are similar. Sleep – or, rather, the lack of it – is a BIG problem for many people.
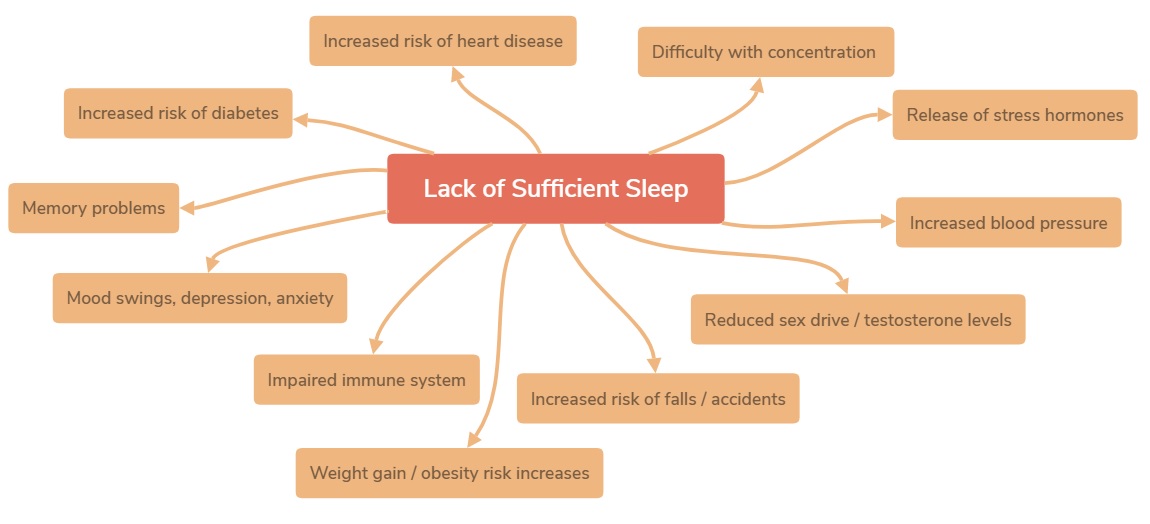
Health conditions associated with lack of sleep
And what few fully appreciate is that blood pressure (BP) rises if you have insufficient sleep. And raised BP is not all. The following are also associated with sleep deficiency:
So, how do we ensure that we stand the best chance of getting enough good quality sleep? The following are associated with improved sleep patterns according to both third-party studies and my own professional/personal experience:
Melatonin is a hormone secreted at night by the pineal gland in the center of our brain to help regulate our circadian rhythm. Supplements are used to prevent and reduce jet lag. MIT got the patent to use melatonin to help people sleep. But melatonin “is not only produced in the pineal gland—it is also naturally present in edible plants.
The above is by no means meant to be a comprehensive list of the chronic health conditions associated with sleep deficiency; nor have I provided a definitive list of suggestions for improving sleep quality. If it forms a basis for discussion or for you to undertake your own research (and send me the findings, please!) then that is a sufficient achievement.
What I will add is that the four cornerstones of health that I continue to mention (diet, sleep, exercise and stress-avoidance) are all a part of the wholistic approach that I consider optimal for human health and well-being.
Diet is perhaps the most important element in all of this, since it forms the basis for being able to sleep well, recover from and endure exercise, and enjoy a positive, stress-reduced mental attitude. Part of the reason why it is able to do this is because it is fundamental to maintaining the body in a state of homeostasis (balance), rather than having to constantly detoxify, protect and repair itself from the inferior “foods” we have so often forced our poor bodies to eat.
Wholistic = Diet+Exercise+Sleep+Stress Reduction…They work together. They compliment one another.
A few final words from Dr Neal Barnard about high-protein foods and sleep
“While many people believe that high-protein meals are key to getting a good night’s rest, the opposite is true. High-protein foods block the brain’s ability to produce serotonin. Because high-protein foods contain more amino acids, tryptophan—the amino acid that eventually turns into serotonin—is crowded out of the brain. As a result, high-protein foods will leave you feeling alert.
High-protein plant-based foods, like tofu, beans, and lentils, are very nutritious. But if you’re having trouble sleeping, try eating these foods earlier in the day. You’ll feel more alert during the day, while favoring carbohydrates later on can help you rest at night.”
Dr Neal Barnard in his own words:
References
Health conditions associated with lack of sleep (in addition to the above links)
Osamu Tochikubo, Akihiko Ikeda, Eiji Miyajima, Masao Ishii. https://doi.org/10.1161/01.HYP.27.6.1318. Hypertension. 1996;27:1318-1324. Originally published June 1, 1996. Effects of Insufficient Sleep on Blood Pressure Monitored by a New Multibiomedical Recorder.
Noguti J, Andersen ML, Cirelli C, Ribeiro DA. Sleep Breath. 2013 Sep;17(3):905-10. doi: 10.1007/s11325-012-0797-9. Epub 2013 Feb 1. Oxidative stress, cancer, and sleep deprivation: is there a logical link in this association?
Redeker NS, Pigeon WR, Boudreau EA. Support Care Cancer. 2015 Apr;23(4):1145-55. doi: 10.1007/s00520-014-2537-0. Epub 2014 Dec 16. Incorporating measures of sleep quality into cancer studies.
Wang P, Ren FM, Lin Y, Su FX, Jia WH, Su XF, Tang LY, Ren ZF. Sleep Med. 2015 Apr;16(4):462-8. doi: 10.1016/j.sleep.2014.11.017. Epub 2015 Feb 3. Night-shift work, sleep duration, daytime napping, and breast cancer risk.
Olsson M, Ärlig J, Hedner J, Blennow K1, Zetterberg H. Sleep. 2018 Feb 7. doi: 10.1093/sleep/zsy025. Sleep Deprivation and CSF Biomarkers for Alzheimer Disease.
Ju YE, McLeland JS, Toedebusch CD, Xiong C, Fagan AM, Duntley SP, Morris JC, Holtzman DM. AMA Neurol. 2013 May;70(5):587-93. doi: 10.1001/jamaneurol.2013.2334. Sleep quality and preclinical Alzheimer disease.
Malhotra RK. Sleep Med Clin. 2018 Mar;13(1):63-70. doi: 10.1016/j.jsmc.2017.09.006. Epub 2017 Nov 10. Neurodegenerative Disorders and Sleep.
Holingue C, Wennberg A, Berger S, Polotsky VY, Spira AP. Metabolism. 2018 Jan 31. pii: S0026-0495(18)30029-5. doi: 10.1016/j.metabol.2018.01.021. Disturbed Sleep and Diabetes: A Potential Nexus of Dementia Risk.
Lao XQ, Liu X, Deng HB, Chan TC, Ho KF, Wang F, Vermeulen R, Tam T, Wong MCS, Tse LA, Chang LY, Yeoh EK. J Clin Sleep Med. 2018 Jan 15;14(1):109-117. doi: 10.5664/jcsm.6894. Sleep Quality, Sleep Duration, and the Risk of Coronary Heart Disease: A Prospective Cohort Study With 60,586 Adults.
Solarz DE, Mullington JM, Meier-Ewert HK. Front Biosci (Elite Ed). 2012 Jun 1;4:2490-501. Sleep, inflammation and cardiovascular disease.
Ancoli-Israel S, DuHamel ER, Stepnowsky C, Engler R, Cohen-Zion M, Marler M. Chest. 2003 Oct;124(4):1400-5. The relationship between congestive heart failure, sleep apnea, and mortality in older men.
Patyar S, Patyar RR.. J Stroke Cerebrovasc Dis. 2015 May;24(5):905-11. doi: 10.1016/j.jstrokecerebrovasdis.2014.12.038. Epub 2015 Mar 25. Correlation between Sleep Duration and Risk of Stroke.
Miller MA, Kruisbrink M, Wallace J, Ji C, Cappuccio FP. Sleep. 2018 Feb 1. doi: 10.1093/sleep/zsy018. Sleep Duration and Incidence of Obesity in Infants, Children and Adolescents: A Systematic Review and Meta-Analysis of Prospective Studies.
Bell JF, Zimmerman FJ. Arch Pediatr Adolesc Med. 2010 Sep;164(9):840-5. doi: 10.1001/archpediatrics.2010.143. Shortened nighttime sleep duration in early life and subsequent childhood obesity.
Hart CN, Jelalian E. Behav Sleep Med. 2008;6(4):251-67. doi: 10.1080/15402000802371379. Shortened sleep duration is associated with pediatric overweight.
Taveras EM, Gilliman MW, Pena MM, Redline S, Rifas Shiman SL. Jun;133(6):1013-22. Pediatrics. 2014. Chronic Sleep Curtailment and Adiposity.
Patel SR, Hu FB. Obesity (Silver Spring). 2008; 16:643-53. Short sleep duration and weight gain: a systematic review.
PatelSR, Malhotra A, White DP, Gottlieb DJ, Hu FB. Am J Epidemiol.2006; 164:947-54. Association between reduced sleep and weight gain in women.
Kim CW, Chang Y, Sung E, Ryu S.. Diabet Med. 2017 Nov;34(11):1591-1598. doi: 10.1111/dme.13432. Epub 2017 Aug 14. Sleep duration and progression to diabetes in people with prediabetes defined by HbA1c concentration.
Briançon-Marjollet A, Weiszenstein M, Henri M, Thomas A, Godin-Ribuot D, Polak J. Diabetol Metab Syndr. 2015 Mar 24;7:25. doi: 10.1186/s13098-015-0018-3. eCollection 2015. The impact of sleep disorders on glucose metabolism: endocrine and molecular mechanisms.
Orzeł-Gryglewska J. Int J Occup Med Environ Health. 2010;23(1):95-114. doi: 10.2478/v10001-010-0004-9. Consequences of sleep deprivation. [Immunological changes]
Riemann D, Baglioni C, Spiegelhalder K. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2011 Dec;54(12):1296-302. doi: 10.1007/s00103-011-1378-y. [Lack of sleep and insomnia. Impact on somatic and mental health]. [Article in German]
Riemann D. Sleep Med. 2007 Dec;8 Suppl 4:S15-20. doi: 10.1016/S1389-9457(08)70004-2. Insomnia and comorbid psychiatric disorders.
Papadimitriou GN, Linkowski P. Int Rev Psychiatry. 2005 Aug;17(4):229-36. Sleep disturbance in anxiety disorders.
Roehrs T, Hyde M, Blaisdell B, Greenwald M, Roth T. Sleep. 2006 Feb;29(2):145-51. Sleep loss and REM sleep loss are hyperalgesic. [Increased cute/chronic pain sensitivity]
Alexandre C, Latremoliere A, Ferreira A, Miracca G, Yamamoto M, Scammell TE, Woolf CJ. Nat Med. 2017 Jun;23(6):768-774. doi: 10.1038/nm.4329. Epub 2017 May 8. Decreased alertness due to sleep loss increases pain sensitivity in mice.
Pastuszak AW, Moon YM, Scovell J, Badal J, Lamb DJ, Link RE, Lipshultz LI. Urology. 2017 Apr;102:121-125. doi: 10.1016/j.urology.2016.11.033. Epub 2016 Dec 14. Poor Sleep Quality Predicts Hypogonadal Symptoms and Sexual Dysfunction in Male Nonstandard Shift Workers.
Hirotsu C, Soterio-Pires JH, Tufik S, Andersen ML. Int J Impot Res. 2017 May;29(3):126. doi: 10.1038/ijir.2017.1. Epub 2017 Feb 16. Sleep disturbance and sexual dysfunction in postmenopausal women.
Opstad PK.. J Clin Endocrinol Metab. 1992 May;74(5):1176-83. Androgenic hormones during prolonged physical stress, sleep, and energy deficiency. 9 [Adrenal & Testicular Androgens]
Sheldon Cohen, PhD, William J. Doyle, PhD, Cuneyt M. Alper, MD, Denise Janicki-Deverts, PhD, and Ronald B. Turner, MD. Arch Intern Med. Author manuscript; available in PMC 2010 Jan 12. Published in final edited form as:Arch Intern Med. 2009 Jan 12; 169(1): 62–67. doi: 10.1001/archinternmed.2008.505. Sleep Habits and Susceptibility to the Common Cold.
Liu TZ, Xu C, Rota M, Cai H, Zhang C, Shi MJ, Yuan RX, Weng H, Meng XY, Kwong JS, Sun X. Sleep Med Rev. 2017 Apr;32:28-36. doi: 10.1016/j.smrv.2016.02.005. Epub 2016 Mar 3. Sleep duration and risk of all-cause mortality: A flexible, non-linear, meta-regression of 40 prospective cohort studies.
Tso W, Rao N, Jiang F, Li AM, Lee SL, Ho FK, Li SL, Ip P. J Pediatr. 2016 Feb;169:266-71. doi: 10.1016/j.jpeds.2015.10.064. Epub 2015 Nov 19. Sleep Duration and School Readiness of Chinese Preschool Children.
Street NW, McCormick MC, Austin SB, Slopen N4 Habre R, Molnar BE. Sleep Health. 2016 Jun;2(2):129-135. doi: 10.1016/j.sleh.2016.03.002. Epub 2016 Apr 18. Sleep duration and risk of physical aggression against peers in urban youth.
Luyster FS, Strollo PJ Jr, Zee PC, Walsh JK; Boards of Directors of the American Academy of Sleep Medicine and the Sleep Research Society. Sleep. 2012 Jun 1;35(6):727-34. doi: 10.5665/sleep.1846. Sleep: a health imperative. [Increased risk of fatal accidents]
Philip P, Akerstedt T. Sleep Med Rev. 2006 Oct;10(5):347-56. Epub 2006 Aug 22. Transport and industrial safety, how are they affected by sleepiness and sleep restriction?
Akerstedt T, Kecklund G, Alfredsson L, Selen J. J Sleep Res. 2007 Dec;16(4):341-5. Predicting long-term sickness absence from sleep and fatigue.
Lim J, Dinges DF. Psychol Bull. 2010 May;136(3):375-89. doi: 10.1037/a0018883. A meta-analysis of the impact of short-term sleep deprivation on cognitive variables.
Esposito MJ, Occhionero M1, Cicogna P. Sleep. 2015 Nov 1;38(11):1823-6. doi: 10.5665/sleep.5172. Sleep Deprivation and Time-Based Prospective Memory.
Lima AM, de Bruin VM, Rios ER, de Bruin PF. Naunyn Schmiedebergs Arch Pharmacol. 2014 May;387(5):399-406. doi: 10.1007/s00210-013-0955-z. Epub 2014 Jan 15. Differential effects of paradoxical sleep deprivation on memory and oxidative stress.
Eun Yeon Joo, Cindy W Yoon, Dae Lim Koo, Daeyoung Kim and Seung Bong Hong/ J Clin Neurol. 2012 Jun;8(2):146-150. English. Published online June 29, 2012. https://doi.org/10.3988/jcn.2012.8.2.146. Adverse Effects of 24 Hours of Sleep Deprivation on Cognition and Stress Hormones.
Suggestions for improving quality of sleep (in addition to the above links)
Nutr Res. 2012 May;32(5):309-19. doi: 10.1016/j.nutres.2012.03.009. Epub 2012 Apr 25. Peuhkuri K, Sihvola N, Korpela R. Diet promotes sleep duration and quality.
St-Onge MP, Roberts A, Shechter A, Choudhury AR. J Clin Sleep Med. 2016 Jan;12(1):19-24. doi: 10.5664/jcsm.5384. Fiber and Saturated Fat Are Associated with Sleep Arousals and Slow Wave Sleep.
G. Howatson, P. G. Bell, J. Tallent, B. Middleton, M. P. McHugh, J. Ellis. Eur J Nutr 2012 51(8):909 – 916. Effect of tart cherry juice (Prunus cerasus) on melatonin levels and enhanced sleep quality.
H.-H. Lin, P.-S. Tsai, S.-C. Fang, J.-F. Liu. Asia Pac J Clin Nutr 2011 20(2):169 – 174. Effect of kiwifruit consumption on sleep quality in adults with sleep problems.
Brand S, Gerber M, Beck J, Hatzinger M, Pühse U, Holsboer-Trachsler E. J Adolesc Health. 2010 Feb;46(2):133-41. doi: 10.1016/j.jadohealth.2009.06.018. Epub 2009 Aug 18. High exercise levels are related to favorable sleep patterns and psychological functioning in adolescents: a comparison of athletes and controls.
Thakkar MM, Sharma R, Sahota P. Alcohol. 2015 Jun;49(4):299-310. doi: 10.1016/j.alcohol.2014.07.019. Epub 2014 Nov 11. Alcohol disrupts sleep homeostasis.
Ebrahim IO, Shapiro CM, Williams AJ, Fenwick PB. Alcohol Clin Exp Res. 2013 Apr;37(4):539-49. doi: 10.1111/acer.12006. Epub 2013 Jan 24. Review. Alcohol and sleep I: effects on normal sleep.
Jeanne F. Duffy, M.B.A., Ph.D.a, and Charles A. Czeisler, Ph.D., M.D. Sleep Med Clin. Author manuscript; available in PMC 2010 Jun 1. Published in final edited form as: Sleep Med Clin. 2009 Jun; 4(2): 165–177. doi: 10.1016/j.jsmc.2009.01.004. Effect of Light on Human Circadian Physiology
Giménez MC, Geerdinck LM, Versteylen M, Leffers P, Meekes GJ, Herremans H, de Ruyter B, Bikker JW, Kuijpers PM, Schlangen LJ. J Sleep Res. 2017 Apr;26(2):236-246. doi: 10.1111/jsr.12470. Epub 2016 Nov 10. Patient room lighting influences on sleep, appraisal and mood in hospitalized people.
Yamauchi M, Jacono FJ, Fujita Y, Kumamoto M, Yoshikawa M, Campanaro CK, Loparo KA, Strohl KP, Kimura H. Sleep Breath. 2014 Dec;18(4):829-35. doi: 10.1007/s11325-014-0951-7. Epub 2014 Feb 13. Effects of environment light during sleep on autonomic functions of heart rate and breathing.
Jones C, Dawson D. Nurs Crit Care. 2012 Sep-Oct;17(5):247-54. doi: 10.1111/j.1478-5153.2012.00501.x. Epub 2012 May 15. Eye masks and earplugs improve patient’s perception of sleep.
Hu RF, Jiang XY, Hegadoren KM, Zhang YH. Crit Care. 2015 Mar 27;19:115. doi: 10.1186/s13054-015-0855-3. Effects of earplugs and eye masks combined with relaxing music on sleep, melatonin and cortisol levels in ICU patients: a randomized controlled trial.
Zaharna M, Guilleminault C. Noise Health. 2010 Apr-Jun;12(47):64-9. doi: 10.4103/1463-1741.63205. Sleep, noise and health: review.
Andrew J.HowellNancy L.DigdonKarenBuro. Personality and Individual Differences (ISSID). Volume 48, Issue 4, March 2010, Pages 419-424. Mindfulness predicts sleep-related self-regulation and well-being.
Huang X, Mazza G. Crit Rev Food Sci Nutr. 2011 Apr;51(4):269-84. doi: 10.1080/10408398.2010.529193. Application of LC and LC-MS to the analysis of melatonin and serotonin in edible plants.
Kehara S, Iso H, Date C, Kikuchi S, Watanabe Y, Wada Y, Inaba Y, Tamakoshi A; JACC Study Group. Association of Sleep Duration with Mortality from Cardiovascular Disease and Other Causes for Japanese Men and Women: the JACC Study. Sleep. 2009 Mar;32(3):295-301.
If you already know about The China Study then you will know how important a milestone it is for nutritional research. It’s such an important study that I thought it would be worth taking a quick look at its background, method and conclusions.
Background
Protein Consumption in Rats
Professor T Colin Campbell observed a relationship between the amount of dietary protein consumed and the promotion of cancer in rats. The animal protein used was casein (the main protein in milk and cheese), along with a variety of plant proteins. Distinct differences between the effects of animal vs. plant-based protein were observed:
animal protein tended to promote disease conditions
plant protein tended to have the opposite effect
Early 1970’s in China
The Chinese premier Zhou Enlai was dying of cancer. He had organised a survey called the Cancer Atlas which gathered details on about 880 million people. The survey revealed cancer rates across China to be geographically localised, suggesting dietary/environmental factors—not genes—accounted for differences in disease rates.
1983-1984 Survey
Dr. Campbell with researchers from Cornell University, Oxford University, and the Chinese government, conducted a major epidemiological study (i.e. a study of human populations to discover patterns of disease and the factors that influence them). This was called The China Project (from which the book The China Study derived some of its data). Researchers investigated the relationship between disease rates and dietary/lifestyle factors across the country.
Why China?
large population of almost one billion
very little migration within China
rural Chinese mostly lived where they were born
strict residential registration system existed
food production was very localised
the Cancer Atlas had revealed diseases were localised and so dietary and environmental factors (not genes) would be likely to account for disease rate variation by area (whether affluent and eating Western diet, or rural and eating traditional plant-based diet)
Method
Research Questions
1. Is there an association between environmental factors, like diet and lifestyle, and risk for chronic disease?
2. Would the patterns observed in a human population be consistent with diet and disease associations observed in experimental animals?
Hypothesis
Researchers hypothesised generally that an association between diet/lifestyle factors and disease rates would indeed exist. A specific hypothesis was that animal product consumption would be associated with an increase in cancer and chronic, degenerative disease.
Hypothesis Testing
6,500 adults in 65 different counties across China were surveyed in the 1983-4 project. These counties represented the range of disease rates countrywide for seven different cancers. The survey process with each participant included:
three-day direct observation
comprehensive diet and lifestyle questionnaires
blood and urine samples
food samples from local markets analysed for nutritional composition
survey of geographic factors
1989-1990 Survey
same counties and individuals resurveyed plus a survey of 20 additional new counties in mainland China and Taiwan.
10,200 adults surveyed
socioeconomic information collected
data combined with new mortality data for 1986-88
Analysis of Data from both 1983-1984 & 1989-1990 Surveys
data was analysed at approximately two dozen laboratories around the world to reduce chances of error in data analysis
researchers could be confident that if results were consistent, then they would be correct
Conclusion
diseases more common in Western countries clustered together geographically in richer areas of China
diseases in richer areas of the world were thus likely to be attributed to similar “nutritional extravagance”
diseases in poorer areas of the world were likely to be attributed to nutritional inadequacy/poor sanitation
blood cholesterol (strongly associated with chronic, degenerative diseases) was higher in those consuming more animal foods
lower oestrogen levels in women (associated with fewer breast cancers) related to increased plant food consumption
higher intake of fibre (found only in plants) associated with lower incidence of colon and rectal cancer
The consistency of the results led the researchers to make the overall conclusion that the closer people came to an all plant-based diet, the lower their risk of chronic disease.
Published Data
The data on both the 1983-1984 survey and the 1989-1990 survey can be seen in more detail here.
More detail on the experimental study design of the China Project (covered in Appendix B) plus a full copy of The China Study in pdf format is available here.
Professor T Colin Campbell’s complete CV (including published papers analysing data from the China Project) is available here.
Plant Protein vs Animal Protein Webinar from Professor T Colin Campbell
If you have any comments or require further information on this topic, please let me know.
Bibliography:
Chen J, Campbell TC, Li J, Peto R. Diet, Life-Style and Mortality in China: A Study of the Characteristics of 65 Chinese Counties. Oxford, UK: Oxford University Press; 1990.
Chen J, Peto R, Pan W-H, Liu B-Q, Campbell TC, Boreham J, Parpia B. Mortality, Biochemistry, Diet and Lifestyle in Rural China: Geographic Study of the Characteristics of 69 Counties in Mainland China and 16 Areas in Taiwan. Oxford, UK; Ithaca, NY; Beijing, PRC: Oxford University Press, Cornell University Press; People’s Medical Publishing House, 1990.
I had a recent email asking me whether there really was any problem with swapping nasty old butter for cholesterol-lowering coconut butter. Well, let’s see, shall we?
“Eating a lot of saturated fat can increase the levels of cholesterol in your blood. Having high cholesterol can increase your risk of heart disease, which includes heart attack and narrowed arteries (atherosclerosis).”
“HEART UK advises people who want to lower their blood cholesterol to avoid using coconut oil in cooking and certainly not use it as a dietary supplement. Creamed and desiccated coconut contain around 60-70% coconut fat should also only be consumed occasionally or in small amounts as part of an overall healthy diet….The Cholesterol Charity wishes to correct the misleading claims being made in the press…claiming coconut oil helps lower blood cholesterol and have even suggested taking coconut oil as a dietary supplement. Coconut oil contains about 85% saturated fatty acids mainly as lauric and myristic acid which potently raise both total cholesterol and low density lipoprotein cholesterol more than other fatty acids (1,2,3,4).”
“…coconut oil. Harmful? Harmless? Or, helpful? In terms of what it does to our cholesterol, it is as harmful as butter.”
PCRM (Physicians Committee for Responsible Medicine)
“According to the American Heart Association, consuming saturated fat raises cholesterol levels in your blood, increasing risk for cardiovascular problems and Alzheimer’s disease. Setting aside saturated fat can also decrease your risk for obesity, diabetes, and cancer.”
“…replacing dietary saturated fats with ‘good carbs’ such as fruits, vegetables, and whole grains, reduced the risk of cardiovascular disease.”
So, in light of the foregoing, does this mean I consider saturated fat and especially coconut oil/butter to be our number one public enemy?
No, not at all.
Focusing on any individual food “fragment”, whether it be a vitamin, mineral or an extracted oil from olives or organic Free Trade coconut butter, is a reductionist approach to nutrition that, in my opinion, is simply misguided. Concentrating on the individual harms or benefits of any individual part of our diet at the expense of stepping back and looking at diet as a whole is the reason that we have drifted into the pandemic of obesity and other diet-related chronic diseases.
Of course, if someone held my arm up my back and forced me to decide whether I would recommend eating coconut butter or an animal butter, I would have to say do NOT eat the animal product; but this would be like forcing me to decide whether I would recommend smoking cigars or smoking pipes! Without any doubt, I would say that it is better to smoke neither.
I believe exactly the same when talking about deciding between animal fats/oils and plant fats/oils – eat neither.
Why would I recommend anything to my clients, family or friends other than the diet that has repeatedly been shown to be the optimal diet for human health and longevity – a whole food plant-based diet.
And the emphasis here in on the word “whole”. The whole plant. Not the oil. The human body understands what a whole food is – it has been surviving and evolving on whole plant foods for millions of years. The body simply does not understand what concentrated and isolated components of plants are, let alone what to do with isolated animal or commercially altered and processed components. The body is used to the whole food (macronutrients, micronutrients and fibre) so that it can digest and absorb what it requires and safely excrete toxins and surplus nutrients as it sees fit.
Shock the system with isolated and concentrated saturated fat, or pretty much any other fragment of food, and the body cannot maintain homeostasis without a cost being paid right down at the cellular level – from the endothelial cells lining blood vessels to adipocytes bulking up that adipose fat around your waist (and your heart!)
“People eat food. Studies focusing on the health impact of differing amounts of saturated fat intake often fail to look at what the subjects are actually eating. Many foods that are low in saturated fat are still unhealthy. Therefore, what you eat instead of foods high in saturated fat is also critical…Not surprisingly, when you replace an unhealthy diet with an unhealthy diet, they both look about the same…if you replace saturated fat with plant-based foods, people do better.”
Replacing unhealthy animal foods with unhealthy plant foods might have some benefits, but you just have to look at an overweight and diabetic vegetarian or vegan to know that jumping out of the BBQ into a deep-fried tofu frying pan is no solution if you want optimal health.
“…animal-based protein is more hazardous than lipids (cholesterol and fatty acids)…Unsaturated fats (PUFAs) are susceptible to tissue damaging oxidation, and saturated fat is not…[which] cause aging and increases cardiovascular disease and cancer…plant oils experimentally promote cancer much more than does saturated fats—that’s right. This is an experimental observation that is at least 30-40 years old…this mainly refers to added oils-isolated from plant sources. It does not refer to the oil within those plant-based foods because plants contain lots of antioxidants to keep the tissue damaging effects of ROS [reactive oxygen species] under control. In my opinion, this is a primary reason for avoiding consumption of added oils. Another reason for avoiding these oils is their contribution to total calorie intake which displaces, in effect, the consumption of calorie-containing whole, plant-based foods.”
So, in summary, my considered opinion is that if a person is really concerned about what food they put in their bodies – if they really want to be healthy and do all they can to weigh the balance in favour of a long and useful life – then forget about debating which food fragment is better than another, just transition to the only diet that has been proven to reverse heart disease and many other chronic diseases – one that is based exclusively on whole food plants.
I will leave the final word on added oil (ANY oils, including coconut oil or coconut butter) to Dr Esselstyn:
References
1. Sundram K, Hayes KC, Siru OH (1994) Dietary Palmitic Acid Results in Lower Serum Cholesterol Than Does a Lauric-Myristic Acid Combination in Normolipemic Humans. Am J Clin Nutr 59, 841-846. 2. Temme EHM, Mensink RP, Hornstra G (1996) Comparison of the effects of diets enriched with lauric, palmitic or oleic acids on serum lipids and lipoproteins in healthy men and women. Am J Clin Nutr 1996; 63: 897-903. 3. Zock P L, de Vries J H, Katan M B (1994) Impact of Myristic versus palmitic acid on serum lipid and lipoproteins levels in health men and women Arterioscler Thromb Vasc Biol 1994;14:567-575. 4. Sanders TA (2013) Reappraisal of SFA and Cardiovascular Risk. Proc Nutr Soc, 72(4), 1-9.
You may never have heard of these two terms, “wholism” and “reductionism”, but the war between them is not just a war of words, it’s a war of paradigms. One of these paradigms is unfortunately winning most of the battles, and the result is an escalating public health crisis.
First, let’s look at what I mean by “paradigm”. A good example is the difference between geocentric and heliocentric world views that came to a head around the 15th-16th centuries. Before the so-called Copernican Revolution (involving intellectual giants such as Nicolaus Copernicus (1473-1543), Johannes Kepler (1571-1630) and Galileo Galilei (1564-1642), the accepted and, for the most part, unchallenged paradigm was that the Sun and other planets revolved around the Earth, and the stars were all fixed in the heavens, just like it said in the Bible. Post-Revoltion, there was a slow but ultimately complete “paradigm shift” which meant that everyone now accepts that the Earth and other planets revolve around the Sun, and the stars are no longer just pin-pricks in some form of heavenly firmament.
Put simply, in terms of nutrition, wholism (a term adopted by Professor T Colin Campbell from the similar and better-known term “holism”) deals with whole diet and its effects on the whole person; whereas reductionism looks at specific elements of diet and their effect on specific parts of the person (like a specific gene for loving or hating Marmite).
The seemingly unstoppable increase in diet-related chronic diseases, such as type 2 diabetes and obesity, is simply not being addressed by the ever more precise research being undertaken by scientists, whether they are chemists looking at a specific chemical that can target particular cellular behaviour or a geneticist looking at which gene is responsible for the onset of a particular disease.
Of course it’s necessary to narrow one’s visual field to a specific area of investigation when it is appropriate (for instance, using a microscope to distinguish which virus has infected a given tissue sample); but there is a general tendency nowadays within nutritional science to exclusively apply the microscope (metaphorically speaking) to every public health issue.
Let’s look at an example: A recent report revealed that half of our schoolchildren are now dangerously overweight or obese.
A reductionist response could be to look for and try and isolate the gene that causes obesity in children. £millions or even £billions could be poured into expensive genetic research to find this “needle in the haystack”. Whereas a wholistic response could be to look at what societal changes have occurred that might account for this unwelcome change in the health of schoolchildren. You don’t have to be a rocket scientist to see that there has been a significant change in the average diets that schoolchildren are now eating when compared to previous generations.
With the reductionist response, one could expect that years and even decades could pass without anything being discovered, and all the while more and more children are likely to become obese.
With the wholistic approach, a solution could theoretically be found very quickly – legislate to improve school meals, increase junk food taxes, ban advertising of unhealthy foods to children, and so forth. The chances are that obesity statistics would start to improve the more practical efforts were made to change laws, educate parents and improve children’s diets. And whilst it might appear that governments do make some moves in this direction, their efforts to implement substantial solutions end up being quasi-wholistic because they are generally hamstrung by the pressure imposed on them by Big Pharma, Big Medicine and Big Agriculture – and the majority of research funding, whether directly or indirectly (e.g. through universities and other institutions), greatly influences which research is most powerfully supported in government circles and reflected in the media to the public.
But even if simple dietary changes could significantly reduce childhood obesity, it would probably not make the reductionists happy. They would still want to delve down into minutiae and find a biological mechanism that could then be controlled somehow, most likely by a drug that could be patented and sold for profit. There is no profit to be made from people simply changing their diets. And there is certainly no profit to be made by pharmaceutical companies or medical organisations from a population full of healthy people.
But let’s say that the geneticists do find a gene that is strongly associated with childhood obesity. It may still take years or decades of research to transfer that information into a fully-tested and certified treatment, probably in the form of a drug. And even if the obesity pill works in the trials they’ve undertaken, there is no guarantee that it will work within the general population, or that it will be free of serious side-effects only apparent years or decades later (remember Thalidomide?), or if it is too expensive for the majority of people to afford or indeed if the percentage improvement attributable to the drug would bear any comparison with the size of improvement made simply by changing dietary intake.
There is nothing wrong with geneticists exploring the fascinating world of genes, nor is there anything wrong with scientists trying to find what makes one person’s personality different from another’s, or any of the other intriguing questions that beg to be researched and answered by the curious and searching human mind.
What IS a problem, though, is when the ONLY approach to solving scientific problems, particularly those directly linked to public health, is an approach which ignores anything that is “fuzzy” and too…well, human! The funding for most of the scientific research that is undertaken nowadays is only available if there is a tangible and clear hope of achieving a binary, black and white result:
1. A always precedes B.
2. B always follows A.
3. There is no C that could also cause B.
Human behaviour and particularly human nutrition on a population-wide level can never conform to this linear causal pattern. Indeed, even one single cell does not and arguably never can be analysed or understood fully by any amount of analysis – just as can be seen in quantum physics (where electrons can exist in two places at the same time – or cease to exist and reappear elsewhere in ways that can never conform to what we think of as causality), the more we delve into our biochemistry, the more we appreciate how much there is that we can never fully know. Just look at the following diagrammatic representation of just the partial metabolic processes involved in one single cell:
Professor T Colin Campbell explains (1.) the dilemma like this:
“The fact that each nutrient passes through such a maze of reaction pathways suggests that each nutrient also is likely to participate in multiple health and disease outcomes. The one nutrient/one disease relationship implied by reductionism, although widely popular, is simply incorrect. Every nutrient-like chemical that enters this complex system of reactions creates a rippling effect that may extend far into the pool of metabolism. And with every bite of food we eat, there are tens and probably hundreds of thousands of food chemicals entering this metabolism pool more or less simultaneously.”
Whilst it is understandable that the human mind is inquisitive and naturally wants to simplify complexity, is it really essential to map the inter-, intra- and extra-cellular labyrinthine world of the 100 trillion cells comprising the human body before we can identify and apply timely solutions to public health issues?
In any event, our cellular make-up is only one aspect of what constitutes the indefinably complex entity that is a human being. Can we truly ever expect to see a cellular or genetic “cog” that explains what it is to be a friend, a lover, a parent? Why we find beauty in a sunset?
Tackling childhood obesity head-on in the messy “real” world of human populations represents the sort of indeterminate complexity that does not attract large government or institutional funding. More effort goes into producing incomprehensibly complex charts such as the one above than goes into practical measures to help children live full and productive lives. This is not to say that scientists, governments and organisations do not care about the lives of real people – particularly real schoolchildren. Rather, my contention is that they are so wrapped up in doing things the way that things have been done for so long (“stuck inside the paradigm”) that they may, in part, genuinely believe that their way is the ONLY way to solve such public health crises.
This is why I believe it is appropriate to apply the term “paradigm” to the general outlook and approach that science and medicine has been immersed in for at least the past 50 years – probably since the joint effects of two discoveries: the so-called completed list of vitamins and the structure of DNA. It is also the reason why incredibly convincing population studies, such as The China Study, come under attack from reductionist thinkers. They attack such wide-scale population studies because there is no single causal link demonstrated. This is even the case when the study identifies significant differences in health markers (e.g. cancer, heart disease and type 2 diabetes) between those Chinese populations eating the traditional plant-based diets and those Chinese populations that have adopted the Standard American Diet (SAD).
There is good reason for this lack of indisputable causality: and the reason is that it is simply impossible to prove a single causal link between health and diet when, as Professor Campbell indicated above, no single nutritional input ever causes just one single biochemical response. But such linear responses are just what scientists have habitually expected to discover when the overriding world-view they have been exposed to all their academic and professional lives aims to reduce all complexity down to minute and simple mechanics.
You will have heard the saying “The whole is greater than the sum of its parts”. Intuitively obvious, but possibly not so in the majority of research laboratories around the world.
The assumption that it should be possible to find such a causal link is based on a mechanistic reductionist ideal of the Universe. The likes of Ray Kurtzweil et al consider that one day we will be able to understand everything about ourselves – biology, emotions, personality – by drilling down deeper and deeper, smaller and smaller into the world of micro and nano particles until we find all the little “cogs” and see how they are all connected. We will then be able to predict all events in the “macro world” and reproduce them in better ways with far more durable materials than human flesh and blood.
Of course we don’t want to return to an age of religion and mysticism, where all events were caused by unknown and unknowable forces, spirits and demons. Where everything in biology and personality could be accounted for by the four humours – blood, yellow bile, black bile, and phlegm! We all enjoy huge benefits from the application of reductionist approaches to finding causes and cures for TB and smallpox, and without this approach doctors might still be delivering babies with unwashed hands after having chopped up cadavers or been to the toilet, or both.
Also, I can see how a reductionist approach can be very attractive. It’s neat and orderly and avoids that great enemy of the reductionist thinker, namely, uncertainty.
But I propose that the answer to childhood obesity is both complex and simple.
It’s simple because all it requires is that we feed our children the natural diet for our species (ideally consisting completely or in the main part of whole plant foods), while ensuring that they get some regular exercise.
It’s complex because WE – our biochemistry, our personalities, our societies – ARE complex.
But effective and timely solutions to childhood obesity and many other public health crises are much more likely to be found with the help of two eyes rather than the help of a two million pound electron microscope.
Ample evidence already points to dietary change being the major factor needed in order to solve this escalating health problem. So much evidence, indeed, that I have not even bothered to list it in this article. Just scan through the databases of the NCBI or NIHR to see that sufficient research already links obesity to diet. But in spite of this, the main thrust of government and medical policy derives from what is called “Gold Standard” research, where the majority of research funding (and resultant credibility) is assigned to randomised controlled trials (RCT’s) that control all potential extraneous biases. And, clearly, you cannot do with when dealing with the nutritional and behavioural diversity that exists in the wider world of society as a whole.
This situation can be further explained by the analogy of an elephant in a room along with 60,000 blind scientists who are each responsible for describing one individual facet in minute detail. They can talk at length about the life-cycle of one of the thousands of species of bacteria colonising a crack between two toes, or churn out publications on the chemical components of a particular pigment within a hair from its tail. Yes, it’s true that they become incredibly expert in their own field of research, but it takes just one non-visually impaired child running into the room to be able to announce that there’s a bleedin’ great elephant standing there!
And to the surprise of the child, these 60,000 blind researchers with one voice ask “what’s an elephant?”
To those who have their eyes open to the whole picture, they can see that our example of childhood obesity is but one of the many chronic health conditions clearly caused by diet, and it’s always the same diet, the one that contains far too much animal protein, saturated fats, salt, sugar and processed junk, and far too little whole plant foods.
Diet is a “zero-sum” affair. Whenever one unhealthy food item goes into your mouth it means that another more healthy food item didn’t. And it is the cumulative effect of this, meal after meal, day after day, year after year that leads inexorably to the near-epidemic diet-related health issues that are starting to bring our hospitals to a standstill.
A fish is hooked, thrown onto land, flops around for a bit in the air and then escapes back into the water. Eager to tell his fishy buddies about his experience, he starts talking to them about his time out of the water. “What’s water?” they all ask, looking at him as though he’s out of his scaly mind. When water is all that you know, there is no word for it…
You may enjoy another view of this issue by Dr. Michael Greger…
Bibliography
Campbell, T. Colin. Whole: Rethinking the Science of Nutrition (p. 97). BenBella Books, Inc.. Kindle Edition.
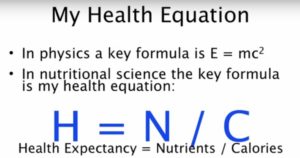

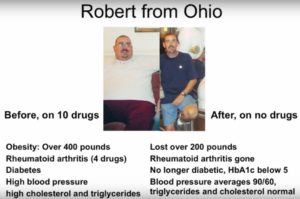

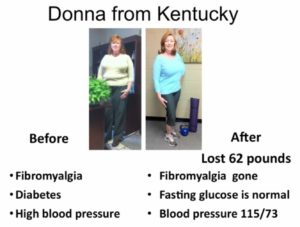
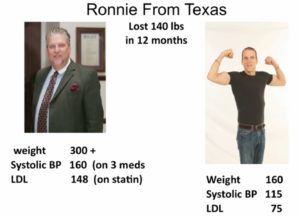
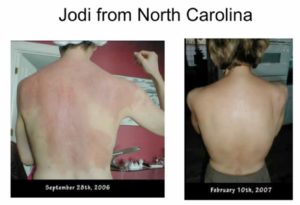
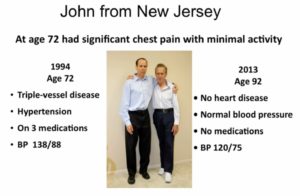

 Joel Fuhrman, M.D. is a board-certified family physician, six-time New York Times best-selling author and internationally recognised expert on nutrition and natural healing.
Joel Fuhrman, M.D. is a board-certified family physician, six-time New York Times best-selling author and internationally recognised expert on nutrition and natural healing.


 First, let me introduce you to someone I expect many of you have never even heard of – Dr Rui Hau Liu, PhD, MD (see bottom of post for more information about his academic and professional qualifications).
First, let me introduce you to someone I expect many of you have never even heard of – Dr Rui Hau Liu, PhD, MD (see bottom of post for more information about his academic and professional qualifications).
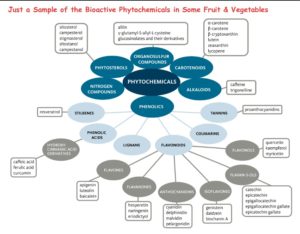 We have little idea yet about how the 8,000 or so known bioactive compounds in fruits, vegetables and whole grains relate to and depend upon each other. And, again, it is thought that there are many thousands more yet to be discovered. It is not, therefore, difficult to understand that food components and nutrients work synergistically in whole foods, through a complex variety of different mechanisms. We cannot replicate the benefits of food with isolated chemical supplements.
We have little idea yet about how the 8,000 or so known bioactive compounds in fruits, vegetables and whole grains relate to and depend upon each other. And, again, it is thought that there are many thousands more yet to be discovered. It is not, therefore, difficult to understand that food components and nutrients work synergistically in whole foods, through a complex variety of different mechanisms. We cannot replicate the benefits of food with isolated chemical supplements.
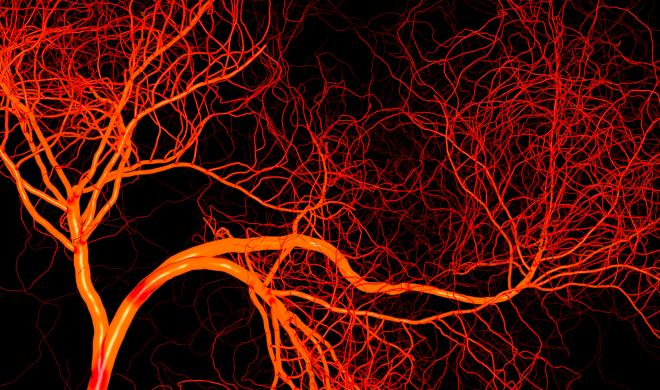

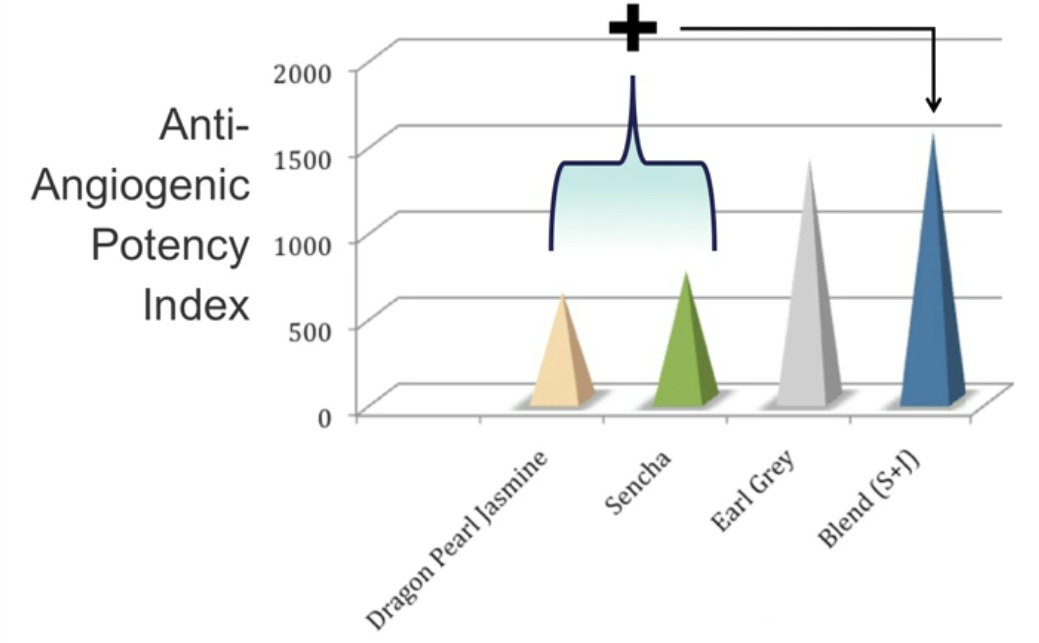
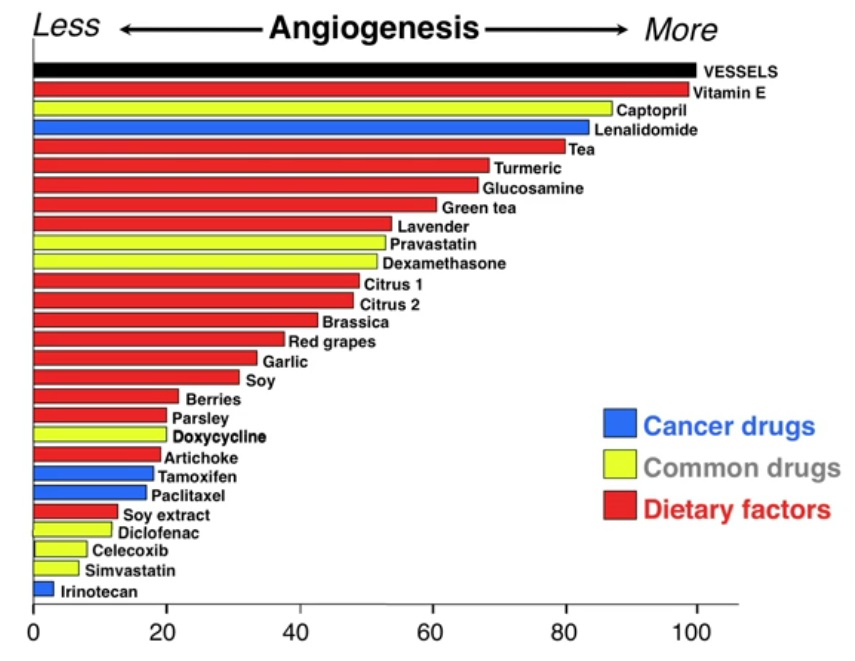 responsible for testing and developing) with the effects of food.
responsible for testing and developing) with the effects of food. A fine example of the
A fine example of the 
 William W. Li is Chief Executive Officer, President, Medical Director, and Co-founder of the Angiogenesis Foundation. Trained in the lab of Dr. Judah Folkman, pioneer of the angiogenesis field, Dr. Li has been actively engaged in angiogenesis research and clinical development for 30 years. Under his leadership, the Foundation has developed a unique social enterprise model based on value creating collaborations with leading medical academic centres, biopharmaceutical and medical device companies, and government agencies, including the National Institutes of Health, Food and Drug Administration, and centres for Medicare and Medicaid Services.
William W. Li is Chief Executive Officer, President, Medical Director, and Co-founder of the Angiogenesis Foundation. Trained in the lab of Dr. Judah Folkman, pioneer of the angiogenesis field, Dr. Li has been actively engaged in angiogenesis research and clinical development for 30 years. Under his leadership, the Foundation has developed a unique social enterprise model based on value creating collaborations with leading medical academic centres, biopharmaceutical and medical device companies, and government agencies, including the National Institutes of Health, Food and Drug Administration, and centres for Medicare and Medicaid Services.