It seems that in many cases, people only take WFPB seriously once they’ve been diagnosed with something really serious, have tried everything else that doctors and faith healers could offer, and then stumble across a website or book advocating a plant-based diet. In their desperation they consider they have nothing to lose – well, nothing except excess fat, toxins, cholesterol, triglycerides, hypertension, inflammation, oxidative stress…
Reactive vs Proactive
We live in a society where you have to get ill before doctors are interested in you. A health system that can only react with pharmaceutical and surgical responses to already developed chronic diseases will only ever succeed in “managing” the symptoms and rarely treat the actual causes.
“The goal of our health system is not health; it’s profit for a few industries at the expense of the public good.”
And the forces that prevent our doctors from being proactive in using preventative rather than reactive medicine are firmly entrenched – both financially and politically.
“Whenever you see large masses of people making what look like “free choices” against their best interests, you can bet that subtle power is at work in the background.”
What a crying shame that our medical professionals and government representatives allow us to get chronically ill in the first place when, for over a century, there’s been powerful evidence that the leading causes of death in western societies can be almost completely avoided by simple dietary/lifestyle changes.
Of course, most of us don’t consider that each time we load processed products and animal foods into our bodies we may as well be loading bullets into a gun pointing straight at our heads. After all, the TV tells us that milk is good for us. The newspapers announce research showing we don’t need to worry about saturated fat any more. Websites reliably inform us that everything is fine in moderation.
“…when we take a step back …we see the mark of a medical industry whose profits depend on doctors’ unquestioning belief and persuasiveness— if not their arrogance.”
And so it comes as a bit of surprise when clothes start to feel tighter, stairs get steeper, breathing seems harder and the doctor informs us that we have diabetes.
“I was only eating what everyone else was eating.”
“The doctor never told me that I could avoid most diseases by eating a plant-based diet.”
“Surely if diet was so important then the government would have put health warnings on the packaging like they have with tobacco!”
Well, it took decades for governments to overcome the financial and political power of the tobacco industry. And Big Food is proving to be even more powerful and cunning than Big Tobacco.
“The structure of the medical industry makes it very difficult for decent and caring doctors to act contrary to the industry’s selfish, profit-seeking, defensive attitude. Those who buck the system face not just ideological pressure, but ideological pressure backed up by the subtle power of money. In some cases, even their license to practice may be challenged.”
What chance does the average person ever have of discovering the truth about diet and health when they are constantly bombarded with misleading signals? Surrounded on every street corner, in every supermarket, even in hospital and school cafeterias with irresistible laboratory-created “foods” that are designed to tempt and addict the unsuspecting consumer After all, the label says it’s low-fat and good for you – full of protein and low in carbs – contains one of your five a day – is fortified with 10 vitamins and minerals.
Doctors receive almost no education on nutrition while they are training. There are no colleges or institutes that can facilitate becoming qualified in plant-based nutrition. The only place (on earth) offering some form of certification is Dr T Colin Campbell’s eCornell plant-based nutrition certificate.
“The medical, pharmaceutical, and supplement industries figured out long ago that a nation of healthy eaters would be disastrous to their profits. They make much more money ignoring and discrediting the evidence for WFPB than by embracing it. So let’s take a look at these three industries and how they maximize profits at the expense of human health.”
I wanted to learn all about nutrition and diet and so worked my way through certificates and diplomas. In order to gain qualifications I had to ‘toe the line’ and churn out all the old stuff about healthy diet meaning oily fish, eggs, milk, lean meat, no processed food and lots of fruit and veg. As part of these courses, I had to learn how to encourage clients to consume the very foods that I knew from my own research would ultimately make them sick. And to practise as a State Registered Dietitian I would have had to spend 3-4 years going through the motions while all the while biting my tongue. I wasn’t prepared to sell my soul in this way.
This must be how certain young doctors may feel if have any idea at all of the preventative power of a plant-based approach to health care. But once qualified, they are tied to the wheel that will roll on and on in the same direction as it has done for decades – controlled by Big Pharma and incapable of straying from the party line, irrespective of what scientific evidence they stumble across on the way.
If you want an expert’s view on the reasons why Big Food, Big Pharma, Big Medicine and Big Government are reluctant to listen to the overwhelming evidence in support of plant-based nutrition as a solution to our chronic disease epidemic, you could do no better than to get hold of a copy of Dr T Colin Campbell’s “Whole“. A handful of quotes from this astonishing book are in bold italics throughout this article.
“But as we’ve seen, that training is limited by the reductionist way we do science. And like any group that “knows best,” doctors can be blind to other options that might be more viable than their own skills and tools. Some of them, out of twin desires to cure and to remain blameless, use their power advantage to bully and silence skeptics who might want to explore wholistic methods of healing. As a result, even the bravest and most open-minded patients usually feel that drugs and surgery are their best bet.”
A Ray of Hope
My previous GP, with whom I’d had some discussions about my own diet, announced to me some time after that he was going to go on a year’s sabbatical to study nutrition. He did this after having made himself aware of the wealth of research supporting a wholly different approach to medicine than the one he was taught.
But I wonder how many other doctors are doing this? He was probably an exception to the rule…
References
All quotes in bold italics are taken from “Whole: Rethinking the Science of Nutrition” (pp. 183, 194/7 & 203/4). Campbell, T. Colin. BenBella Books, Inc.. Kindle Edition.
If you’re already aware of the overwhelming evidence showing the power of a plant-based diet to prevent and treat chronic diseases such as CVD (cardiovascular disease), do you ever wonder why on earth your family doctor, oncologist or cardiologist don’t recommend making simple dietary changes?
A big part of the answer is to do with human nature. Those qualified in modern medicine will have spent almost a decade studying pharmaceutical and surgical solutions and spent only a few academic hours looking at diet – even though overwhelming evidence has existed for over a century that dietary changes can prevent, halt and even reverse some chronic diseases.
If you’d devoted time, effort and money to qualifying as a medical expert in the above way, you wouldn’t want to be told that diseases like CVD, cancer, hypertension, obesity and diabetes can be avoided and dealt with by simply swapping broccoli for your bacon and eggs!
I came across the reality of this in practice quite recently while spending time in hospital as my mother was dying of urinary sepsis with other nasty complications – largely related to poor dietary and exercise choices. Chatting with nurses and doctors reaffirmed my suspicion that those “looking after” our health are more or less ignorant of all the research relating to plant-based diets and their power in preventing and treating disease. They go along with it to a certain extent (“…eat more fruit and veg and less red meat“) but treat any further claims as a joke.
Does this surprise you? If not, then maybe it’s more shocking than if it did surprise you.
Have we become so passive in our acceptance of the ignorance of those to whom we entrust the health of our loved ones that we just expect them – our doctors and surgeons – to continue handing out statins while not even enquiring about why the patient is obese? Offering stents and bypass surgery rather than advising the patient to replace the meat, dairy and eggs with beans, fruit and nuts? Worse than this, they are totally dismissive, and have even been known to refuse treatment, if the patient wants to try WFPB before having their chest ripped open and radioactive chemicals injected into their veins.
Sometimes, I slip into the above passivity and resign myself to the fact that we “WFPBers” are simply out of sync with the world. But at other times, a wave of outrage overwhelms me – particularly when I see a hospital ward full of elderly people who are dying ahead of time because of horrible diseases that could have been largely avoided if only their medical experts had advised them decades ago to cut out the foods that will damage their bodies.
I have studied and written about paradigms. The current medical paradigm involves a reductionist approach to research and treatment. I understand, therefore, that each successive generation of newly-qualified doctors has to appease their superiors and adhere to the methods and approaches they were taught.
I understand that there is much more emphasis on reductionist research rather than on population-wide research – the former is very specific and attracts huge funding; the latter can appear wishy-washy and so attracts almost no funding.
I know it’s human nature to do what you’re told. To practice a profession or trade in the way you were taught, even if there is new information that contradicts the “accepted” tenets you had drilled into your head during your hard-earned education. Equally, it’s clear that young doctors have to tow the line and not contradict their superiors or rock the boat with new ideas. And who would want to spend years training as a cardiologist to then find down the line that there were not enough patients to treat because people were eating foods that kept their hearts healthy?
There’s also the “hypocrisy barrier” to overcome. Which doctor can advise a patient to go home and eat beans and greens when they themselves are likely to pop in for burger on the way home? And this is not a trivial matter. Cast you mind back to how difficult it must have been for doctors to advise patients to quit smoking when they had their own packet of Benson & Hedges on the desk, sitting next to the stethoscope.
Financial profit within the paradigm of the current medical system cannot come from making people too healthy. It requires us to be ill – not too dead but also not too alive.
[su_quote]I hope we shall crush in its birth the aristocracy of our monied corporations which dare already to challenge our government to a trial of strength, and to bid defiance to the laws of their country. —THOMAS JEFFERSON [/su_quote]
And doctors who advocate a plant-based diet – how do they make a living in the our pharmaceutical-led health system? Where’s the profit in giving your patients a prescription to eat more fruit and veg and cut out animal and processed foods?
One of the greatest levers of power we have as individuals in our digital world is to access and read the facts-based research – past, present and future – that vindicates plant-based nutrition as a major solution to most of our chronic diseases. It’s all there on Pubmed, a continually-updated resource of published and peer-reviewed research papers from around the world, including an increasing number that relate to the benefits of a plant-based diet.
And this is the wonderful thing about the WFPB movement – hyperbole is not required. The facts speak for themselves. There is a wealth of research showing the health benefits of simple dietary change. But, unfortunately, for the vast majority of the medical profession, “simple” or “wholistic” solutions (even though shown to be highly effective) do not have the credibility of the more traditional pharmaceutical and surgical approaches which are not appearing to reduce the numbers of people ballooning in size and decaying from within.
It would be far too simplistic to put our health epidemic down to the toxic food choices we are being led to make – even if it were a completely credible explanation.
We need to make a fresh start and take a proactive approach to healthcare instead of a reactive one. We wait to be ill before the medical profession is interested in us. And even when the early stages of disease are detected, pills and potions are recommended as a knee-jerk response, rather than advising timely dietary and lifestyle changes.
We are dealing with the symptoms and not the cause. It’s like going to the doctor with a bad headache because we keep banging it against the wall. The doctor hands us paracetamols and advises the use of an expensive crash helmet, rather than calmly advising us to just stop the head-banging.
[su_quote]Doctors are the clergy for a secular age.—Dr T Colin Campbell[/su_quote]
A single publication by Dr Kim A Williamset al is outlined below. It re-emphasises the need for the medical profession to take seriously the assertion that plant-based diets are a key adjunct in the prevention and treatment of diseases such as CVD. The list of research associated with this publication is also listed below.
Plant-Based Nutrition: An Essential Component of Cardiovascular Disease Prevention and Management. October 2017.
Major points from the research abstract:
Discussion of nutrition and the benefits of a plant-based diet should be highlighted during healthcare provider visits as an essential part of the overall CVD prevention and management care plan.
Evidence from prospective cohort studies indicates that a high consumption of predominantly plant-based foods, such as fruit and vegetables, nuts, and whole grains, is associated with a significantly lower risk of CVD.
The protective effects of these foods are likely mediated through their multiple beneficial nutrients, including mono- and polyunsaturated fatty acids, omega-3 fatty acids, antioxidant vitamins, minerals, phytochemicals, fibre, and plant protein.
Minimising intake of animal proteins has been shown to decrease the prevalence of CVD risk factors.
Substantial evidence indicates that plant-based diets can play an important role in preventing and treating CVD and its risk factors.
Such diets deserve more emphasis in dietary recommendations.
**************************
It may be worth your while spending a little while scanning through the list of research papers below (some particularly relevant ones marked in red type) and, if you have a spare hour or two, delve a little deeper into some of the research that already shows both the damage caused by an animal food-based diet and the health-giving power of a plant-based diet.
It’s great to see luminaries such as Dr Williams passing on the advice of a very wise old medical expert, who said centuries ago “Let food be thy medicine, and medicine thy food.”
References
(Taken from the above-mentioned publication by Dr Kim A Williams et al.)
Celermajer DS, Chow CK, Marijon E, Anstey NM, Woo KS. Cardiovascular disease in the developing world: prevalences, patterns, and the potential of early disease detection. J Am Coll Cardiol. 2012;60(14):1207–16.PubMedCrossRefGoogle Scholar
Mozaffarian D. Dietary and policy priorities for cardiovascular disease, diabetes, and obesity. Circulation. 2016;133(2):187–225.PubMedPubMedCentralCrossRefGoogle Scholar
Heron M, Anderson R. Changes in the leading cause of death: recent patterns in heart disease and cancer mortality. NCHS data brief. 2016;254:1-8.Google Scholar
Tuso PJ, Ismail MH, Ha BP, Bartolotto C. Nutritional update for physicians: plant-based diets. Perm J. 2013;17(2):61–6.PubMedPubMedCentralCrossRefGoogle ScholarThis paper states: “Physicians should consider recommending a plant-based diet to all their patients, especially those with high blood pressure, diabetes, cardiovascular disease, or obesity.”
Hu FB. The Mediterranean diet and mortality—olive oil and beyond. N Engl J Med. 2003;348(26):2595–6.PubMedCrossRefGoogle Scholar
Hu FB, Cespedes Feliciano EM. What should cardiologists tell their patients about a healthy dietary pattern? J Am Coll Cardiol. 2016;68(8):815–7.PubMedCrossRefGoogle Scholar
Willett WC, Sacks F, Trichopoulou A, Drescher G, Ferro-Luzzi A, Helsing E, et al. Mediterranean diet pyramid: a cultural model for healthy eating. Am J Clin Nutr. 1995;61(6 Suppl):1402S–6S.PubMedGoogle Scholar
Epstein FH, Ross R. Atherosclerosis—an inflammatory disease. N Engl J Med. 1999;340(2):115–26.CrossRefGoogle Scholar
Boyle J. Macrophage activation in atherosclerosis: pathogenesis and pharmacology of plaque rupture. Curr Vasc Pharmacol. 2005;3(1):63–8.PubMedCrossRefGoogle Scholar
Vita JA. Polyphenols and cardiovascular disease: effects on endothelial and platelet function. Am J Clin Nutr. 2005;81(1 Suppl):292S–7S.PubMedGoogle Scholar
Esselstyn CB. Resolving the coronary artery disease epidemic through plant-based nutrition. Prev Cardiol. 2001;4(4):171–7.PubMedCrossRefGoogle Scholar
Ornish D. Intensive lifestyle changes for reversal of coronary heart disease. JAMA. 1998;280(23):2001. PubMedCrossRefGoogle Scholar
Hertog MG, Sweetnam PM, Fehily AM, Elwood PC, Kromhout D. Antioxidant flavonols and ischemic heart disease in a Welsh population of men: the Caerphilly study. Am J Clin Nutr. 1997;65(5):1489–94.PubMedGoogle Scholar
Mukamal KJ. Tea consumption and mortality after acute myocardial infarction. Circulation. 2002;105(21):2476–81.PubMedCrossRefGoogle Scholar
Zamora-Ros R, Rabassa M, Cherubini A, Urpi-Sarda M, Bandinelli S, Ferrucci L, et al. High concentrations of a urinary biomarker of polyphenol intake are associated with decreased mortality in older adults. J Nutr. 2013;143(9):1445–50.PubMedPubMedCentralCrossRefGoogle Scholar
Carmeli E, Fogelman Y. Antioxidant effect of polyphenolic glabridin on LDL oxidation. Toxicol Ind Health. 2009;25(4–5):321–4.PubMedCrossRefGoogle Scholar
Frémont L, Belguendouz L, Delpal S. Antioxidant activity of resveratrol and alcohol-free wine polyphenols related to LDL oxidation and polyunsaturated fatty acids. Life Sci. 1999;64(26):2511–21.PubMedCrossRefGoogle Scholar
Bernstein AM, Sun Q, Hu FB, Stampfer MJ, Manson JE, Willett WC. Major dietary protein sources and risk of coronary heart disease in women. Circulation. 2010;122(9):876–83.PubMedPubMedCentralCrossRefGoogle Scholar
Ashaye A, Gaziano J, Djoussé L. Red meat consumption and risk of heart failure in male physicians. Nutr Metab Cardiovasc Dis. 2011 Dec;21(12):941–6.PubMedCrossRefGoogle Scholar
Koeth RA, Wang Z, Levison BS, Buffa JA, Org E, Sheehy BT, et al. Intestinal microbiota metabolism of l-carnitine, a nutrient in red meat, promotes atherosclerosis. Nat Med. 2013;19(5):576–85.PubMedPubMedCentralCrossRefGoogle Scholar
Tang WHW, Wang Z, Levison BS, Koeth RA, Britt EB, Fu X, et al. Intestinal microbial metabolism of phosphatidylcholine and cardiovascular risk. N Engl J Med. 2013;368(17):1575–84.PubMedPubMedCentralCrossRefGoogle Scholar
Yang S-Y, Zhang H-J, Sun S-Y, Wang L-Y, Yan B, Liu C-Q, et al. Relationship of carotid intima-media thickness and duration of vegetarian diet in Chinese male vegetarians. Nutr Metab (Lond). 2011;8(1):63.CrossRefGoogle Scholar
Wang Z, Klipfell E, Bennett BJ, Koeth R, Levison BS, DuGar B, et al. Gut flora metabolism of phosphatidylcholine promotes cardiovascular disease. Nature. 2011;472(7341):57–63.PubMedPubMedCentralCrossRefGoogle Scholar
Kahleova H, Matoulek M, Malinska H, Oliyarnik O, Kazdova L, Neskudla T, et al. Vegetarian diet improves insulin resistance and oxidative stress markers more than conventional diet in subjects with type 2 diabetes. Diabet Med. 2011;28(5):549–59.PubMedPubMedCentralCrossRefGoogle Scholar
De Natale C, Annuzzi G, Bozzetto L, Mazzarella R, Costabile G, Ciano O, et al. Effects of a plant-based high-carbohydrate/high-fiber diet versus high-monounsaturated fat/low-carbohydrate diet on postprandial lipids in type 2 diabetic patients. Diabetes Care. 2009 Dec;32(12):2168–73.PubMedPubMedCentralCrossRefGoogle Scholar
Jiang R, Manson JE, Stampfer MJ, Liu S, Willett WC, Hu FB. Nut and peanut butter consumption and risk of type 2 diabetes in women. JAMA. 2002;288(20):2554–60.PubMedCrossRefGoogle Scholar
Mishra S, Xu J, Agarwal U, Gonzales J, Levin S, Barnard ND. A multicenter randomized controlled trial of a plant-based nutrition program to reduce body weight and cardiovascular risk in the corporate setting: the GEICO study. Eur J Clin Nutr. 2013;67(7):718–24.PubMedPubMedCentralCrossRefGoogle Scholar
Ramal E, Champlin A, Bahjri K. Impact of a plant-based diet and support on mitigating type 2 diabetes mellitus in Latinos living in medically underserved areas. Am J Health Promot. 2017 Jan;1:890117117706793.Google Scholar
Goff LM, Bell JD, So P-W, Dornhorst A, Frost GS. Veganism and its relationship with insulin resistance and intramyocellular lipid. Eur J Clin Nutr. 2005 Feb;59(2):291–8.PubMedCrossRefGoogle Scholar
Virkamäki A, Korsheninnikova E, Seppälä-Lindroos A, Vehkavaara S, Goto T, Halavaara J, et al. Intramyocellular lipid is associated with resistance to in vivo insulin actions on glucose uptake, antilipolysis, and early insulin signaling pathways in human skeletal muscle. Diabetes. 2001 Oct;50(10):2337–43.PubMedCrossRefGoogle Scholar
Tonstad S, Butler T, Yan R, Fraser GE. Type of vegetarian diet, body weight, and prevalence of type 2 diabetes. Diabetes Care. 2009 May;32(5):791–6.PubMedPubMedCentralCrossRefGoogle Scholar
Meyer KA, Kushi LH, Jacobs DR, Slavin J, Sellers TA, Folsom AR. Carbohydrates, dietary fiber, and incident type 2 diabetes in older women. Am J Clin Nutr. 2000 Apr;71(4):921–30.PubMedGoogle Scholar
Stampfer MJ, Hu FB, Manson JE, Rimm EB, Willett WC. Primary prevention of coronary heart disease in women through diet and lifestyle. N Engl J Med. 2000 Jul 6;343(1):16–22.PubMedCrossRefGoogle Scholar
Satija A, Bhupathiraju, S, Spiegelman D, Chiuve S, Manson J, Willett W, Rexrode K, Rimm E, Hu F. Healthful and Unhealthful Plant-Based Diets and the Risk of Coronary Heart Disease. J Am Coll Cardiol. 2017;70:411–22.Google Scholar
Rinaldi S, Campbell EE, Fournier J, O’Connor C, Madill J. A comprehensive review of the literature supporting recommendations from the Canadian Diabetes Association for the use of a plant-based diet for management of type 2 diabetes. Can J Diabetes. 2016;40(5):471–7.PubMedCrossRefGoogle Scholar
Marathe PH, Gao HX, Close KL. American Diabetes Association standards of medical care in diabetes 2017. J Diabetes. 2017;9(4):320–4.PubMedCrossRefGoogle Scholar
Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, et al. Heart disease and stroke statistics—2017 update: a report from the American Heart Association. Circulation. 2017;135(10):e146–603.PubMedPubMedCentralCrossRefGoogle Scholar
Midgley JP, Matthew AG, Greenwood CM, Logan AG. Effect of reduced dietary sodium on blood pressure: a meta-analysis of randomized controlled trials. JAMA. 275(20):1590–7.Google Scholar
Appel LJ, Moore TJ, Obarzanek E, Vollmer WM, Svetkey LP, Sacks FM, et al. A clinical trial of the effects of dietary patterns on blood pressure. N Engl J Med. 1997;336(16):1117–24.PubMedCrossRefGoogle Scholar/ This study concludes that “A diet rich in fruits, vegetables, and low-fat dairy foods and with reduced saturated and total fat can substantially lower blood pressure. This diet offers an additional nutritional approach to preventing and treating hypertension.”
John JH, Ziebland S, Yudkin P, Roe LS, Neil HAW. Oxford fruit and vegetable study group. Effects of fruit and vegetable consumption on plasma antioxidant concentrations and blood pressure: a randomised controlled trial. Lancet (London, England). 2002;359(9322):1969–74.CrossRefGoogle Scholar
Steffen LM, Kroenke CH, Yu X, Pereira MA, Slattery ML, Van Horn L, et al. Associations of plant food, dairy product, and meat intakes with 15-y incidence of elevated blood pressure in young black and white adults: the Coronary Artery Risk Development in Young Adults (CARDIA) study. Am J Clin Nutr. 2005;82(6):1169–77-4.PubMedGoogle Scholar
Borgi L, Curhan GC, Willett WC, Hu FB, Satija A, Forman JP. Long-term intake of animal flesh and risk of developing hypertension in three prospective cohort studies. J Hypertens. 2015 Nov;33(11):2231–8.PubMedPubMedCentralCrossRefGoogle Scholar
Yokoyama Y, Nishimura K, Barnard ND, Takegami M, Watanabe M, Sekikawa A, et al. Vegetarian diets and blood pressure: a meta-analysis. JAMA Intern Med. 2014 Apr;174(4):577–87.PubMedCrossRefGoogle Scholar
National Cholesterol Education Program, National Heart, Lung, and Blood Institute NI of H. Third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III) final report. NIH Publ No 02–5215. 2002;Google Scholar
Jenkins DJA. Effects of a dietary portfolio of cholesterol-lowering foods vs lovastatin on serum lipids and C-reactive protein. JAMA. 2003 Jul 23;290(4):502.PubMedCrossRefGoogle Scholar
Institute of Medicine. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids. Washington, DC: Natl Acad Press. 2005. https://doi.org/10.17226/10490.
Weggemans RM, Zock PL, Katan MB. Dietary cholesterol from eggs increases the ratio of total cholesterol to high-density lipoprotein cholesterol in humans: a meta-analysis. Am J Clin Nutr. 2001 May;73(5):885–91.PubMedGoogle Scholar
Hopkins PN. Effects of dietary cholesterol on serum cholesterol: a meta-analysis and review. Am J Clin Nutr. 1992 Jun;55(6):1060–70.PubMedGoogle Scholar
•• Song M, Fung TT, Hu FB, Willett WC, Longo VD, Chan AT, et al. Association of animal and plant protein intake with all-cause and cause-specific mortality. JAMA Intern Med. 2016;176(10):1453. This study showed that high animal protein intake was positively associated with cardiovascular mortality, and high plant protein intake was inversely associated with all-cause and cardiovascular mortality, especially among individuals with at least 1 lifestyle risk factor. Thus, substituting plant protein for animal protein, especially from processed red meat, was associated with lower mortality, highlighting the importance of protein source.PubMedCrossRefPubMedCentralGoogle Scholar
Shin JY, Xun P, Nakamura Y, He K. Egg consumption in relation to risk of cardiovascular disease and diabetes: a systematic review and meta-analysis. Am J Clin Nutr. 2013 Jul;98(1):146–59.PubMedPubMedCentralCrossRefGoogle Scholar
Wang F, Zheng J, Yang B, Jiang J, Fu Y, Li D. Effects of vegetarian diets on blood lipids: a systematic review and meta-analysis of randomized controlled trials. J Am Heart Assoc. 2015 Oct 27;4(10):e002408.PubMedPubMedCentralCrossRefGoogle Scholar
Mensink RP, Zock PL, Kester ADM, Katan MB. Effects of dietary fatty acids and carbohydrates on the ratio of serum total to HDL cholesterol and on serum lipids and apolipoproteins: a meta-analysis of 60 controlled trials. Am J Clin Nutr. 2003 May;77(5):1146–55.PubMedGoogle Scholar
Eckel RH, Jakicic JM, Ard JD, de Jesus JM, Houston Miller N, Hubbard VS, et al. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk. J Am Coll Cardiol. 2014 Jul;63(25):2960–84.PubMedCrossRefGoogle Scholar
Agriculture. UD of H and HSUD of. 2015–2020 Dietary Guidelines for Americans. 8th ed. [Internet]. Washington, DC: US Dept of Health and Human Services. 2015. http://www.health.gov/DietaryGuidelines. 1 Jun (2017).
Agudo A, Cabrera L, Amiano P, Ardanaz E, Barricarte A, Berenguer T, et al. Fruit and vegetable intakes, dietary antioxidant nutrients, and total mortality in Spanish adults: findings from the Spanish cohort of the European Prospective Investigation into Cancer and Nutrition (EPIC-Spain). Am J Clin Nutr. 2007 Jun;85(6):1634–42.PubMedGoogle Scholar
Chrysohoou C, Panagiotakos DB, Pitsavos C, Das UN, Stefanadis C. Adherence to the Mediterranean diet attenuates inflammation and coagulation process in healthy adults: the ATTICA study. J Am Coll Cardiol. 2004 Jul 7;44(1):152–8.PubMedCrossRefGoogle Scholar
Dai J, Jones DP, Goldberg J, Ziegler TR, Bostick RM, Wilson PW, et al. Association between adherence to the Mediterranean diet and oxidative stress. Am J Clin Nutr. 2008 Nov;88(5):1364–70.PubMedPubMedCentralGoogle Scholar
Zino S, Skeaff M, Williams S, Mann J. Randomised controlled trial of effect of fruit and vegetable consumption on plasma concentrations of lipids and antioxidants. BMJ. 1997 Jun 21;314(7097):1787–91.PubMedPubMedCentralCrossRefGoogle Scholar
• Wolk A. Potential health hazards of eating red meat. J Intern Med. 2017;281(2):106–22. This review examined the correlation between disease risk and meat consumption in six cohort studies to provide a comprehensive summary of the potential negative health effects of consuming red meat, including significantly increased risks for diabetes, heart disease, stroke, and cancer.PubMedCrossRefGoogle Scholar
Buckland G, González CA, Agudo A, Vilardell M, Berenguer A, Amiano P, et al. Adherence to the Mediterranean diet and risk of coronary heart disease in the Spanish EPIC cohort study. Am J Epidemiol. 2009;170(12):1518–29.PubMedCrossRefGoogle Scholar
Fung TT, Rexrode KM, Mantzoros CS, Manson JE, Willett WC, Hu FB. Mediterranean diet and incidence of and mortality from coronary heart disease and stroke in women. Circulation. 2009;119(8):1093–100.PubMedPubMedCentralCrossRefGoogle Scholar
Mitrou PN, Kipnis V, Thiébaut ACM, Reedy J, Subar AF, Wirfält E, et al. Mediterranean dietary pattern and prediction of all-cause mortality in a US population: results from the NIH-AARP diet and health study. Arch Intern Med. 2007;167(22):2461–8.PubMedCrossRefGoogle Scholar
Sofi F, Abbate R, Gensini GF, Casini A. Accruing evidence on benefits of adherence to the Mediterranean diet on health: an updated systematic review and meta-analysis1. Am J Clin Nutr. 2010;92(5):1189–96.PubMedCrossRefGoogle Scholar
Sofi F, Cesari F, Abbate R, Gensini GF, Casini A. Adherence to Mediterranean diet and health status: meta-analysis. BMJ. 2008;337:a1344.PubMedPubMedCentralCrossRefGoogle Scholar
•• Åkesson A, Larsson SC, Discacciati A, Wolk A. Low-risk diet and lifestyle habits in the primary prevention of myocardial infarction in men. J Am Coll Cardiol. 2014;64(13):1299–306. This study showed that the risk of myocardial infarction is significantly reduced by adherence to very basic lifestyle modifications. PubMedCrossRefGoogle Scholar
Estruch R, Ros E, Salas-Salvadó J, Covas M-I, Corella D, Arós F, et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N Engl J Med. 2013;368(14):1279–90.PubMedCrossRefGoogle Scholar
Nagura J, Iso H, Watanabe Y, Maruyama K, Date C, Toyoshima H, et al. Fruit, vegetable and bean intake and mortality from cardiovascular disease among Japanese men and women: the JACC study. Br J Nutr. 2009;102(2):285–92.PubMedCrossRefGoogle Scholar
Strandhagen E, Hansson PO, Bosaeus I, Isaksson B, Eriksson H. High fruit intake may reduce mortality among middle-aged and elderly men. The study of men born in 1913. Eur J Clin Nutr. 2000;54(4):337–41.PubMedCrossRefGoogle Scholar
Bazzano LA, He J, Ogden LG, Loria CM, Vupputuri S, Myers L, et al. Fruit and vegetable intake and risk of cardiovascular disease in US adults: the first national health and nutrition examination survey epidemiologic follow-up study. Am J Clin Nutr. 2002;76(1):93–9.PubMedGoogle Scholar
Wang X, Ouyang Y, Liu J, Zhu M, Zhao G, Bao W, et al. Fruit and vegetable consumption and mortality from all causes, cardiovascular disease, and cancer: systematic review and dose-response meta-analysis of prospective cohort studies. BMJ. 2014 Jul 29;349:g4490.PubMedPubMedCentralCrossRefGoogle Scholar
He FJ, Nowson CA, MacGregor GA. Fruit and vegetable consumption and stroke: meta-analysis of cohort studies. Lancet (London, England). 2006;367(9507):320–6.CrossRefGoogle Scholar
Chowdhury R, Warnakula S, Kunutsor S, Crowe F, Ward HA, Johnson L, et al. Association of dietary, circulating, and supplement fatty acids with coronary risk: a systematic review and meta-analysis. Ann Intern Med. 2014;160(6):398–406.PubMedCrossRefGoogle Scholar
Yakoob MY, Shi P, Hu FB, Campos H, Rexrode KM, Orav EJ, et al. Circulating biomarkers of dairy fat and risk of incident stroke in U.S. men and women in 2 large prospective cohorts. Am J Clin Nutr. 2014;100(6):1437–47.PubMedPubMedCentralCrossRefGoogle Scholar
Kelemen LE, Kushi LH, Jacobs DR, Cerhan JR. Associations of dietary protein with disease and mortality in a prospective study of postmenopausal women. Am J Epidemiol. 2005;161(3):239–49.PubMedCrossRefGoogle Scholar
Chen M, Sun Q, Giovannucci E, Mozaffarian D, Manson JE, Willett WC, et al. Dairy consumption and risk of type 2 diabetes: 3 cohorts of US adults and an updated meta-analysis. BMC Med. 2014;12:215.PubMedPubMedCentralCrossRefGoogle Scholar
Zong G, Li Y, Wanders AJ, Alssema M, Zock PL, Willett WC, et al. Intake of individual saturated fatty acids and risk of coronary heart disease in US men and women: two prospective longitudinal cohort studies. BMJ. 2016;355:i5796.PubMedPubMedCentralCrossRefGoogle Scholar
Harris WS, Mozaffarian D, Rimm E, Kris-Etherton P, Rudel LL, Appel LJ, et al. Omega-6 fatty acids and risk for cardiovascular disease: a science advisory from the American Heart Association Nutrition Subcommittee of the Council on Nutrition, Physical Activity, and Metabolism; Council on Cardiovascular Nursing; and Council on Epidem. Circulation. 2009;119(6):902–7.PubMedCrossRefGoogle Scholar
Ramsden CE, Zamora D, Majchrzak-Hong S, Faurot KR, Broste SK, Frantz RP, et al. Re-evaluation of the traditional diet-heart hypothesis: analysis of recovered data from Minnesota coronary experiment (1968-73). BMJ. 2016;353:i1246.PubMedPubMedCentralCrossRefGoogle Scholar
Ramsden CE, Zamora D, Leelarthaepin B, Majchrzak-Hong SF, Faurot KR, Suchindran CM, et al. Use of dietary linoleic acid for secondary prevention of coronary heart disease and death: evaluation of recovered data from the Sydney diet heart study and updated meta-analysis. BMJ. 2013;346:e8707.PubMedPubMedCentralCrossRefGoogle Scholar
Hamazaki T, Okuyama H. The Japan Society for Lipid Nutrition recommends to reduce the intake of linoleic acid. A review and critique of the scientific evidence. World Rev Nutr Diet. 2003;92:109–32.PubMedCrossRefGoogle Scholar
Nielsen MS, Schmidt EB, Stegger J, Gorst-Rasmussen A, Tjonneland A, Overvad K. Adipose tissue arachidonic acid content is associated with the risk of myocardial infarction: a Danish case-cohort study. Atherosclerosis. 2013 Apr;227(2):386–90.PubMedCrossRefGoogle Scholar
Farvid MS, Ding M, Pan A, Sun Q, Chiuve SE, Steffen LM, et al. Dietary linoleic acid and risk of coronary heart disease: a systematic review and meta-analysis of prospective cohort studies. Circulation. 2014 Oct 28;130(18):1568–78.PubMedPubMedCentralCrossRefGoogle Scholar
Jakobsen MU, O’Reilly EJ, Heitmann BL, Pereira MA, Bälter K, Fraser GE, et al. Major types of dietary fat and risk of coronary heart disease: a pooled analysis of 11 cohort studies. Am J Clin Nutr. 2009 May;89(5):1425–32.PubMedPubMedCentralCrossRefGoogle Scholar
Li Y, Hruby A, Bernstein AM, Ley SH, Wang DD, Chiuve SE, et al. Saturated fats compared with unsaturated fats and sources of carbohydrates in relation to risk of coronary heart disease: a prospective cohort study. J Am Coll Cardiol. 2015 Oct 6;66(14):1538–48.PubMedPubMedCentralCrossRefGoogle Scholar
Craig WJ. Mangels, AR ADA. Position of the American dietetic association: vegetarian diets. J Am Diet Assoc. 2009 Jul;109(7):1266–82.PubMedCrossRefGoogle Scholar
Young VR, Pellett PL. Plant proteins in relation to human protein and amino acid nutrition. Am J Clin Nutr. 1994 May;59(5 Suppl):1203S–12S.PubMedGoogle Scholar
Wilson AK, Ball MJ. Nutrient intake and iron status of Australian male vegetarians. Eur J Clin Nutr. 1999 Mar;53(3):189–94.PubMedCrossRefGoogle Scholar
Waldmann A, Koschizke JW, Leitzmann C, Hahn A. Dietary iron intake and iron status of German female vegans: results of the German vegan study. Ann Nutr Metab. 2004 Apr 21;48(2):103–8.PubMedCrossRefGoogle Scholar
Etemadi A, Sinha R, Ward MH, Graubard BI, Inoue-Choi M, Dawsey SM, Abnet CC. Mortality from different causes associated with meat, heme iron, nitrates, and nitrites in the NIH-AARP Diet and Health Study: population based cohort study. BMJ. 2017 May 9;357:j1957. https://doi.org/10.1136/bmj.j1957.
Hunt JR. Moving toward a plant-based diet: are iron and zinc at risk? Nutr Rev. 2002 May 1;60(5):127–34.PubMedCrossRefGoogle Scholar
Haddad EH, Berk LS, Kettering JD, Hubbard RW, Peters WR. Dietary intake and biochemical, hematologic, and immune status of vegans compared with nonvegetarians. Am J Clin Nutr. 1999 Sep;70(3 Suppl):586S–93S.PubMedGoogle Scholar
Appleby P, Roddam A, Allen N, Key T. Comparative fracture risk in vegetarians and nonvegetarians in EPIC-Oxford. Eur J Clin Nutr. 2007 Dec 7;61(12):1400–6.PubMedCrossRefGoogle Scholar
Davey GK, Spencer EA, Appleby PN, Allen NE, Knox KH, Key TJ. EPIC–Oxford:lifestyle characteristics and nutrient intakes in a cohort of 33 883 meat-eaters and 31 546 non meat-eaters in the UK. Public Health Nutr. 2003 Jun;2:6(3).Google Scholar
Trang HM, Cole DE, Rubin LA, Pierratos A, Siu S, Vieth R. Evidence that vitamin D3 increases serum 25-hydroxyvitamin D more efficiently than does vitamin D2. Am J Clin Nutr. 1998 Oct;68(4):854–8.PubMedGoogle Scholar
Šebeková K, Boor P, Valachovičová M, Blažíček P, Parrák V, Babinská K, et al. Association of metabolic syndrome risk factors with selected markers of oxidative status and microinflammation in healthy omnivores and vegetarians. Mol Nutr Food Res. 2006 Sep;50(9):858–68.PubMedCrossRefGoogle Scholar
Donaldson MS. Metabolic vitamin B12 status on a mostly raw vegan diet with follow-up using tablets, nutritional yeast, or probiotic supplements. Ann Nutr Metab. 2000 Dec 27;44(5–6):229–34.PubMedCrossRefGoogle Scholar
Brug J. Determinants of healthy eating: motivation, abilities and environmental opportunities. Fam Pract. 2008;25(Supplement 1):i50–5.PubMedCrossRefGoogle Scholar
Janssen M, Busch C, Rödiger M, Hamm U. Motives of consumers following a vegan diet and their attitudes towards animal agriculture. Appetite. 2016 Oct 1;105:643–51.PubMedCrossRefGoogle Scholar
Fox N, Ward K. Health ethics and environment: a qualitative study of vegetarian motivations. Appetite. 2008 Mar;50(2–3):422–9.PubMedCrossRefGoogle Scholar
We are constantly bombarded by new claims about the benefits of taking this or that supplement. The implicit assumption made by this emphasis on supplementation is that a varied and healthy diet alone can’t supply everything that the body needs to maintain homeostasis – that is, its optimal natural balance. I want to challenge this assumption and put whole plant foods back at the top of the Must Have list…
First, let me introduce you to someone I expect many of you have never even heard of – Dr Rui Hau Liu, PhD, MD (see bottom of post for more information about his academic and professional qualifications).
Dr Liu makes it makes it clear that the majority of all the current and past scientific evidence suggests that it is the whole plant food approach, and not the dietary supplement approach, that is the powerful solution for cancer prevention and health promotion. He points out that a dietary supplement (which might contain one compound or multiple compounds) “… cannot mimic a natural combination of the bioactive compound in foods, vegetables, and whole grains.” And the scientific literature suggests that “…the single antioxidant, single bioactive compound approach is not working. For example, beta carotene, selenium, vitamin E and vitamin C alone to prevent cancer is not as effective as a combination of the compound from the whole fruit.” (From a lecture in Diseases of Affluence module 2.16 of the eCornell Certificate in Plant Based Nutrition.)
His advice is that, instead of trusting expensive dietary supplements, we should eat a wide variety of fruits, vegetables, whole grains and other plant-based foods – whether these be processed, raw, cooked, dried, fresh, canned, frozen or in the form of 100% whole plant juices. The important thing is to increase the plant-based portion sizes that we consume. Some bioactive compounds are more bioavailable without processing, and some others are more bioavailable after cooking. For instance, the antioxidant benefits of the lycopene in tomatoes increases after cooking.
Dr Liu looked at whole plant food consumption compared with supplements. His team increased the number of apples (from 1 to 6 apples per day) fed to study animals. While the supplements had little or no effect (and in some of his studies, injurious effects), apples both inhibited tumour appearance and caused existing tumours to grow more slowly. The thing here is that it is not an isolated component of the food item (in this case apple) that can be extracted and made to be useful; rather, it has to be a matter of taking nature’s “medicine” in whole natural form, so that our bodies can absorb and utilise the bioactive components.
This then permits all the hugely complex range of bioactive compounds to come into play – many, perhaps the vast majority of which, we do not yet even know. These include secondary metabolites and antioxidants such as the carotenoids, phenolic acids, and flavonoids and many other compounds.
To illustrate this, here are just a few of the known bioactive components within just six divisions of the flavanoid group:
There are many other flavonoids, including some of the more common ones called aurones, xanthones, and condensed tannins.
We have little idea yet about how the 8,000 or so known bioactive compounds in fruits, vegetables and whole grains relate to and depend upon each other. And, again, it is thought that there are many thousands more yet to be discovered. It is not, therefore, difficult to understand that food components and nutrients work synergistically in whole foods, through a complex variety of different mechanisms. We cannot replicate the benefits of food with isolated chemical supplements.
The complexity is simply mind-boggling and will probably always be beyond our minds to comprehend, and our scientific instruments to measure. However, we would be able to see the results in those individuals and populations whose habitual diets consist largely or exclusively of whole plant foods.
Evolutionary processes, over vast aeons of time, have equipped plants with intricate and highly effective defences against everything from damaging sunlight radiation and hungry insects, to fungi, viruses and bacteria. And, slowly but surely, evolution has also established mechanisms through which our human bodies are able to access and extract these bioactive plant compounds and, thus, take advantage of their beneficial properties.
So, the next time we are encouraged to buy the latest miracle dietary supplement, perhaps we’ll give it a miss – we get enough a mouthful of miracles every time we bite into a juicy apple.
Dr Rui Hau Liu, PhD, MD
Rui Hai Liu is a Professor in the Department of Food Science at Cornell University. He received his PhD in Toxicology from Cornell University in 1993. He also holds a MD in Medicine and a MS in Nutrition and Food Toxicology. Dr Liu was a Research Associate in the Department of Clinical Sciences in the College of Veterinary Medicine at Cornell University.
His research program focuses on diet and cancer, effect of functional foods/nutraceuticals on chronic disease risks, and bioactive compounds in natural products and herbal remedies for anticancer and antiviral activity.
His specific interests include:
1) health benefits of phytochemicals in fruits, vegetables, and whole grains;
2) food genomics and functional foods for disease prevention and health promotion targeted at cancers, aging, and inflammatory diseases; and
3) natural products and herbal formulations for antiviral activity to hepatitis B and C.
Thomson Reuters recognized Liu as one of the world’s most influential scientific minds for 2014 and 2015 and named him as a highly cited researcher.
He has published more than 145 scientific papers in peer-reviewed journals and accrued over 11,100 citations. Essential Science Indicators ranked him as one of the top five scientists in the field of agricultural sciences, including nutrition and food science. In 2011, he received the Institute of Food Technologists’ Babcock-Hart Award for outstanding contributions to the field of food science in the improvement of public health through nutrition.
Note: For more information on Dr. Rui Hai Liu’s work visit Cornell University.
References
Boyer J, Liu RH. Nutr J. 2004; 3(5). Apple phytochemicals and their health benefits.
Ali Ghasemzadeh. Neda Ghasemzadeh. Journal of Medicinal Plants Research Vol. 5(31), pp. 6697-6703, 23 December, 2011. Available online at http://www.academicjournals.org/JMPR. Flavonoids and phenolic acids: Role and biochemical activity in plants and human.
Campbell TC, Jacobson H. Benbella Books, Dallas TX. 2013. Whole: Rethinking the Science of Nutrition.
Eberhardt MV, Lee CY, Liu RH. Nature. 2000 Jun 22; 405(6789): 903-4. Antioxidant activity of fresh apples.
Liu RH, Liu J, Chen B. J Agric Food Chem. 2005; 53:2341-2343. Apples prevent mammary tumors in rats.
Science Watch Author Commentaries. (2012). http://archive.sciencewatch.com/inter/aut/2012/12-jan/12janLiu/. Rui Hai Liu on studying the health benefits of whole foods.
Dean Ornish et al. https://www.ornish.com/wp-content/uploads/8369.full_.pdf?4ae29f. Changes in prostate gene expression in men undergoing an intensive nutrition and lifestyle intervention.
Dean Ornish. https://www.ornish.com/wpcontent/uploads/Intensive_Lifestyle_Changes_and_Prostate_Cancer.pdf?4ae29f. Intensive Lifestyle Changes May Affect the Progression of Prostate Cancer.
David Palma, Tom Pickles. https://www.ornish.com/wp-content/uploads/telomerase-benefits-healthy-living1.pdf?4ae29f. Telomerase and the benefi ts of healthy living.
T Colin Campbell. https://nutritionstudies.org/mystique-of-protein-implications/. The Mystique of Protein and Its Implications.
Preventative Medicine Research Institute. http://www.pmri.org/
Video recorded at UR Nutrition in Medicine’s Lunch with Docs on April 8th, 2017. Nutrition and Cancer, Lecture from Dr. Thomas Campbell
The 1958 Delaney Amendment stated that “…no additive is deemed safe if it is found [in “appropriate” tests] to induce cancer when ingested by man or animal…” This US amendment required zero tolerance – that is, no amount of any substance found to be carcinogenic could be added to food. Of course, we know that this noble goal was never achieved and now we have carcinogenic food additives and carcinogenic food processing methods.
£billions are spent researching potential carcinogens found in the environment rather than those found in food. Why is this? Simply, it is easier to get funding for this type of reductionist research than it is to deal with the complexities of human nutrition on a population-wide basis. Also, the so-called Toxic Triad of Big Food, Big Farming and Big Pharma put political and commercial pressure (and lots of it) on research institutions to avoid pointing the finger at powerful food manufacturers, distributors and sellers who make huge profits and contribute huge sums to both government and academic institutions around the world.
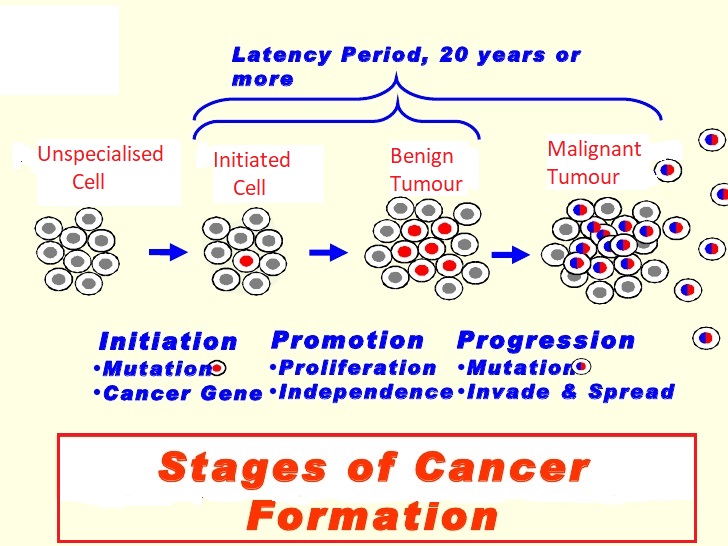
The three phases of cancer
Also, there has been an overwhelming emphasis on the first phase of the three phases of cancer (Initiation, Promotion & Progression).
Genetic science appears to be somewhat hamstrung by a particular paradigm. Within this paradigm, consideration is almost solely given to the concept that the only approach we can take is to try and prevent cancers by avoiding the Initiation stage (which happens in a tiny fraction of a second) when DNA is first exposed to carcinogens at the point of cellular reproduction. Once the cancer has passed to the Promotion (years to decades) or Progression (usually years) stages, the seemingly unchallenged consensus appears to be that there is no point in doing anything other than turn to one of the three ugly sisters – surgery, radiation or chemotherapy. As we will see later, there is strong evidence that cancer can be slowed, halted and even reversed completely throughout the Promotion stage and, to perhaps a lesser degree, in the Progression stage of cancer development.
Much of the focus of scientific research, government legislation and media coverage is on individual non-dietary carcinogens (such as radon or asbestos). And even when researchers do deal with diet-related carcinogens, the emphasis for most part is on those carcinogens that are unintentionally included in the food cycle (such as aflatoxin in corn and peanut mould or 2,3,7,8-Tetrachlorodibenzodioxin which is produced during the manufacture of chlorinated hydrocarbons). This tendency can be seen, for instance, in this quote from a section entitled Types of Food Contaminants (my bold highlighted text) in a peer-reviewed paper entitled “Carcinogenic Food Contaminants”:
“There are four primary types of potentially carcinogenic compounds that have been examined to determine if they act as carcinogens in humans. The first are natural products that may be present in food and are unavoidable. For example, the process of creating salted fish produces carcinogens which can not be easily avoided. Second, are natural products that might be avoided such as the contamination of grain with the carcinogenic fungal metabolite aflatoxin, which can be reduced or eliminated using best practices for grain storage. Third, anthropogenic chemicals may be present in food. For instance, 2,3,7,8-tetracholordibenzo-p-dioxin has been inadvertently produced during the manufacture of chlorinated hydrocarbons, but it contaminates the environment, resists degradation, and accumulates in certain foodstuffs. A fourth category of concern is anthropogenic chemicals intentionally added to foods, such as saccharin or food coloring, but these are not addressed in this review because they are not contaminants because they are added intentionally.”
It may be an erroneous assumption, but could this stated avoidance of investigating those dietary carcinogens “intentionally” added to our food be motivated by hidden political/commercial pressures to do so? The paper continues (my bold highlighted text) to this conclusion:
“The accumulation of evidence sufficient to render judgement on food contaminants and human cancer risk is a daunting task…several food contaminants have been confirmed as carcinogenic to humans. Possibly the clearest example is the finding that aflatoxin is a major cause of liver cancer…”
Again, we see a tendency to seek the “clearest” (read “easiest to research”) examples of dietary carcinogens as well as a tendency to miss the elephant in the room – namely, the fact that ALL cancers and other diet-related chronic diseases (e.g. heart disease, diabetes, obesity) are rising around the world at a pace perfectly in parallel with the equal rise in adoption of the Standard American Diet (SAD).
There are reported to be between 80,000 and 100,000 environmental chemicals that would need to be thoroughly tested in order to establish whether or not they each represent a significant cancer risk for humans. Imagine how long that would take? As research teams trawl through these, the focus on the avoidable (i.e. both those intentionally avoided “intentionally added”) dietary carcinogens referred to above would continue to be unwittingly consumed by millions of people. And this is aside from those carcinogens that are not added to foods, but actually ARE the foods, such as our next and main topic casein in dairy.
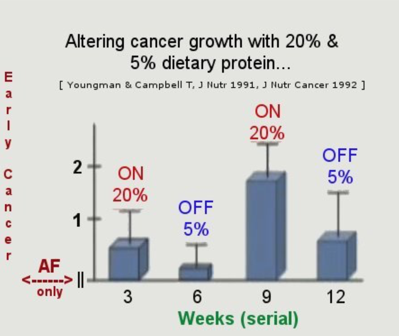
The animal protein used by Professor T Colin Campbell and his team of researchers was casein, which represents around 85% of all the protein in cow’s milk. He demonstrated that you could turn cancer tumours on and off in rats and mice merely by alternating the amount of protein consumed from 5% to 20% and then from 20% back down to 5% of their total daily calorie intake. Since this research, which is now decades old, he was able to identify the precise mechanisms concerned and how they are involved in all three phases of cancer development.
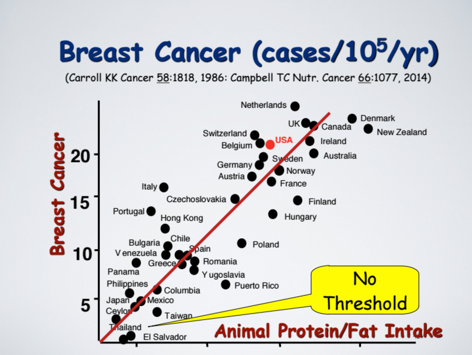
He is also convinced that other animal proteins have the same detrimental effects – that is, if animal protein intake is increased then cancer risk also increases; but if animal protein intake is reduced then the cancer risk decreases. This can be witnessed in human populations. The following graph shows the example of breast cancer and its geographical spread by country and quantity of average national levels of animal protein (and in this case, also animal fat) consumption. The USA is highlighted in red, but the UK has even higher incidence of breast cancer per capita, reflecting the corresponding higher protein (and fat) intake.
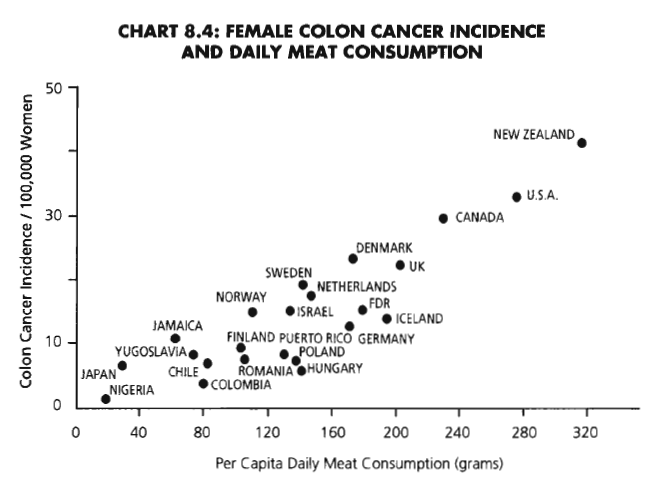
The following chart from The China Study shows female colon cancer rising with meat consumption.
And just to hammer home the correlation between animal protein consumption and incidence of cancer, I have included these further charts from other research:
Assuming a causal rather than a merely correlational relationship between these factors, we can identify the particular protein’s amino acid composition as the specific reason for the adverse effects. Sufficient studies for more than 50 years have shown that the nutritional responses of different proteins are attributed to their differing amino acid compositions; and the differences in nutritional response between animal and plant proteins disappear when any limiting amino acids are restored. Limiting amino acids are those essential amino acids which are present in only small quantities within any given food. The only “food” completely lacking one essential amino acid is gelatin which completely lacks tryptophan. All other foods, as far as I am aware, contain all the essential amino acids, but – and this is the significant point – in varying amounts.
Throughout many experiments over a period of over 30 years, Professor Campbell’s research team found that casein in particular was a powerful promoter of cancer, with two of the major contributory factors being:
increased production of growth hormones, and
elevated body acid load (metabolic acidosis).
Unlike animal proteins such as casein, plant proteins (for instance, the protein in wheat) does not stimulate cancer development. However, as indicated above – when wheat’s limiting amino acid, lysine, is restored to the relevant level, wheat protein acts just the same as casein in terms of cancer promotion.
So, to recap:
animal and plant proteins are not the same
the variation is due to their different amino acid compositions
these different amino acid compositions produce different nutritional responses.
While animal proteins do vary between themselves, any difference is much less than the degree to which they differ from plant proteins as a whole, and there is virtually no overlap between the two groups of protein.
The conventional way in which the so-called “quality” or “completeness” of a protein is determined relates to protein’s efficiency ratio. Thus, plant proteins are described as having LBV (Low Biological Value) while animal proteins are HBV (High Biological Value) depending on how many grams of gain in body weight occur with a given intake of the protein:
Animal proteins cause a greater weight gain over a specified period of time
Plant proteins cause a lesser weight gain over a specified period of time.
Thus,
Egg, meat, cow’s milk, and fish promote a faster rate of growth
Rice, beans and wheat flour promote a slower rate of gain.
So what’s wrong with that?
Nothing, if you want your farm animals to grow rapidly to return the maximum profit over the shortest time; but not if you are a human. Rapid growth in childhood is not a beneficial thing and rapid growth of cancer cells in childhood or adulthood is generally accepted as undesirable.
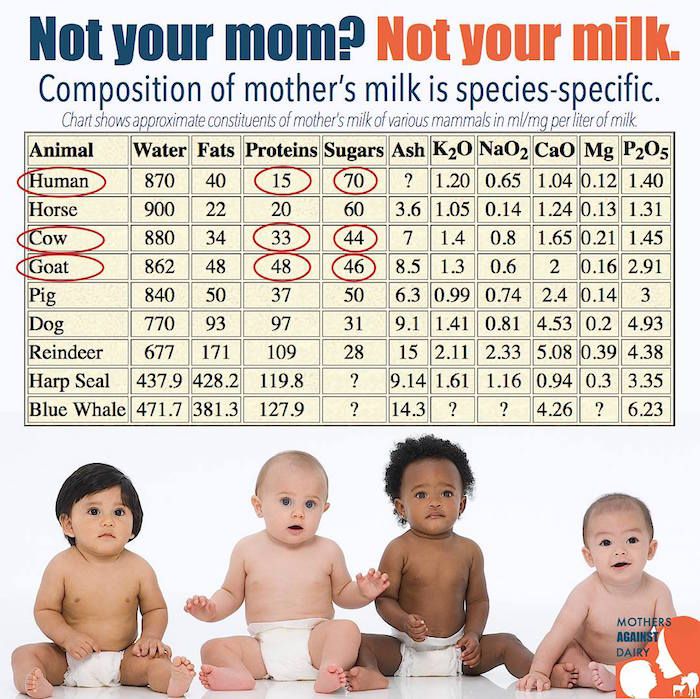
Cow’s Milk is Baby Calf Growth Fluid
And, as Dr Michael Klaper says: “The purpose of cow’s milk is to turn a 65-pound calf into a 700-pound cow as rapidly as possible. Cow’s milk IS baby calf growth fluid. No matter what you do to it, that is what the stuff is.”
It appears at first sight to be a truly shocking that Professor Campbell should define casein in dairy as “The most relevant cancer promoter ever discovered.”
But it is possible to understand this when one considers the increasingly ubiquitous role that dairy plays in the majority of diets. Dairy products are in everything from pizzas to puddings, sherbets to soups. I needn’t tell you how much the dairy industry promotes its supposed (and largely discredited) health benefits – you just need to turn on the TV or flick through a magazine. And the public at large are so taken in by the claims that it is good for your bones (debatable) and or that it is a health food (debatable).
Dr Neil Barnard from the PCRM (Physicians Committee for Responsible Medicine) goes just as far as Professor Campbell and Dr Michael Klaper. He says “Thanks to these marketing campaigns, milk myths abound in our culture. But science doesn’t support them.” Calling them “white lies” he goes on to attack the myths that the milk industry continues to promote to the public. (Click picture below to read his article, “White Lies? Five Milk Myths Debunked”.)
It occurred to me that one of the reasons that the dairy industry peddles the unsubstantiated myth about milk’s bone-building features is that it is a useful distraction from the potentially catastrophic impact of casein. Maybe I’m just being cynical…In any case, here’s Dr Michael Greger’s view on milk and bone health:
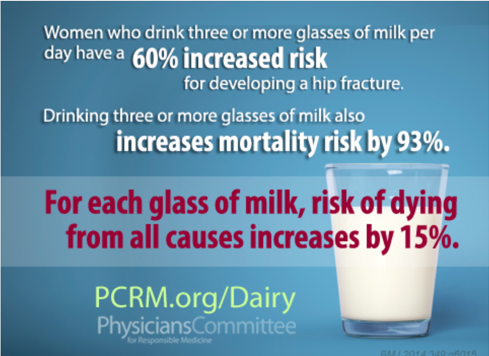
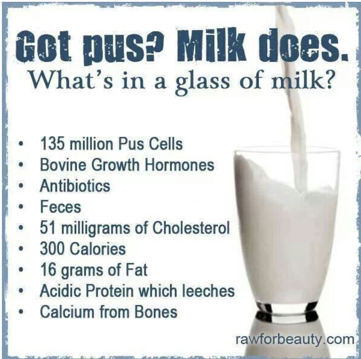
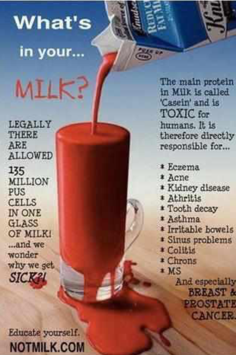
Finally, if you are still in doubt about whether or not people are wise to pour a bit of the white (or red) stuff into their breakfast cereal, I will leave you with a couple of self-explanatory posters about a rather distasteful ingredient that you won’t hear the dairy industry mooing about…
References
T. Colin Campbell. J Nat Sci. Author manuscript; available in PMC 2017 Oct 18. Published in final edited form as: J Nat Sci. 2017 Oct; 3(10): e448. Cancer Prevention and Treatment by Wholistic Nutrition.
David O. Carpenter M.D., Sheila Bushkin-Bedient M.D. Journal of Adolescent Health. Volume 52, Issue 5, Supplement, May 2013, Pages S21-S29. Exposure to Chemicals and Radiation During Childhood and Risk for Cancer Later in Life.
Campbell TC. J Nat Sci. 2017 Oct;3(10). pii: e448. Cancer Prevention and Treatment by Wholistic Nutrition.
Campbell TC. Nutr Cancer. 2017 Aug-Sep;69(6):962-968. doi: 10.1080/01635581.2017.1339094. Epub 2017 Jul 25. Nutrition and Cancer: An Historical Perspective.-The Past, Present, and Future of Nutrition and Cancer. Part 2. Misunderstanding and Ignoring Nutrition.
Campbell TC. Nutr Cancer. 2017 Jul;69(5):811-817. doi: 10.1080/01635581.2017.1317823. Epub 2017 Jun 8. The Past, Present, and Future of Nutrition and Cancer: Part 1-Was A Nutritional Association Acknowledged a Century Ago?
Campbell TM, Campbell TC. Isr Med Assoc J. 2008 Oct;10(10):730-2. The benefits of integrating nutrition into clinical medicine.
Sarter B, Campbell TC, Fuhrman J. Altern Ther Health Med. 2008 May-Jun;14(3):48-53. Effect of a high nutrient density diet on long-term weight loss: a retrospective chart review.
Campbell TC. MedGenMed. 2007;9(3):57. Fail to test the impressive ability of diet to favorably affect long-term health and body weight loss.
Campbell TC. Am J Clin Nutr. 2007 Jun;85(6):1667. Dietary protein, growth factors, and cancer.
Wang Y, Crawford MA, Chen J, Li J, Ghebremeskel K, Campbell TC, Fan W, Parker R, Leyton J. Comp Biochem Physiol A Mol Integr Physiol. 2003 Sep;136(1):127-40. Fish consumption, blood docosahexaenoic acid and chronic diseases in Chinese rural populations.
Feskanich D, Bischoff-Ferrari HA, Frazier AL, Willett WC. JAMA Pediatr. 2014 Jan;168(1):54-60. doi: 10.1001/jamapediatrics.2013.3821. Milk consumption during teenage years and risk of hip fractures in older adults.
Sun Z, Zhang Z, Wang X, Cade R, Elmir Z, Fregly M. Peptides. 2003 Jun;24(6):937-43. Relation of beta-casomorphin to apnea in sudden infant death syndrome.
Fiedorowicz E, Jarmołowska B, Iwan M, Kostyra E, Obuchowicz R, Obuchowicz M. Peptides. 2011 Apr;32(4):707-12. The influence of μ-opioid receptor agonist and antagonist peptides on peripheral blood mononuclear cells (PBMCs).
Kost NV, Sokolov OY, Kurasova OB, Dmitriev AD, Tarakanova JN, Gabaeva MV, Zolotarev YA, Dadayan AK, Grachev SA, Korneeva EV, Mikheeva IG, Zozulya AA. Peptides. 2009 Oct;30(10):1854-60. Beta-casomorphins-7 in infants on different type of feeding and different levels of psychomotor development.
A S Wiley. Biol. 2012 Mar-Apr;24(2):130-8. Cow milk consumption, insulin-like growth factor-I, and human biology: a life history approach. Am J Hum
B C Melnik, S M John, G Schmitz. Nutr J. 2013; 12: 103. Milk is not just food but most likely a genetic transfection system activating mTORC1 signaling for postnatal growth.
C Melnik. J Obes. 2012;2012:197653. Excessive Leucine-mTORC1-Signalling of Cow Milk-Based Infant Formula: The Missing Link to Understand Early Childhood Obesity.
M S Kramer. J Pediatr. 1981 Jun;98(6):883-7. Do breast-feeding and delayed introduction of solid foods protect against subsequent obesity?
B C Melnik. World J Diabetes. 2012 Mar 15;3(3):38-53. Leucine signaling in the pathogenesis of type 2 diabetes and obesity.
A S Wiley. PLoS One. 2011 Feb 14;6(2):e14685. Milk intake and total dairy consumption: associations with early menarche in NHANES 1999-2004.
D S Ludwig, W C Willett. JAMA Pediatr. 2013 Sep;167(9):788-9. Three daily servings of reduced-fat milk: an evidence-based recommendation?
K Arnberg, C Molgaard, K F Michaelsen, S M Jensen, E Trolle, A Larnkjaer. J Nutr. 2012 Dec;142(12):2083-90. Skim milk, whey, and casein increase body weight and whey and casein increase the plasma C-peptide concentration in overweight adolescents.
P Wilde, E Morgan, J Roberts, A Schpok, T Wilson. Physiol Behav. 2012 Aug 20;107(1):172-5. Relationship between funding sources and outcomes of obesity-related research.
Youngman LD, Campbell TC. J Nutr. 1991 Sep;121(9):1454-61. High protein intake promotes the growth of hepatic preneoplastic foci in Fischer #344 rats: evidence that early remodeled foci retain the potential for future growth.
If you already know about The China Study then you will know how important a milestone it is for nutritional research. It’s such an important study that I thought it would be worth taking a quick look at its background, method and conclusions.
Background
Protein Consumption in Rats
Professor T Colin Campbell observed a relationship between the amount of dietary protein consumed and the promotion of cancer in rats. The animal protein used was casein (the main protein in milk and cheese), along with a variety of plant proteins. Distinct differences between the effects of animal vs. plant-based protein were observed:
animal protein tended to promote disease conditions
plant protein tended to have the opposite effect
Early 1970’s in China
The Chinese premier Zhou Enlai was dying of cancer. He had organised a survey called the Cancer Atlas which gathered details on about 880 million people. The survey revealed cancer rates across China to be geographically localised, suggesting dietary/environmental factors—not genes—accounted for differences in disease rates.
1983-1984 Survey
Dr. Campbell with researchers from Cornell University, Oxford University, and the Chinese government, conducted a major epidemiological study (i.e. a study of human populations to discover patterns of disease and the factors that influence them). This was called The China Project (from which the book The China Study derived some of its data). Researchers investigated the relationship between disease rates and dietary/lifestyle factors across the country.
Why China?
large population of almost one billion
very little migration within China
rural Chinese mostly lived where they were born
strict residential registration system existed
food production was very localised
the Cancer Atlas had revealed diseases were localised and so dietary and environmental factors (not genes) would be likely to account for disease rate variation by area (whether affluent and eating Western diet, or rural and eating traditional plant-based diet)
Method
Research Questions
1. Is there an association between environmental factors, like diet and lifestyle, and risk for chronic disease?
2. Would the patterns observed in a human population be consistent with diet and disease associations observed in experimental animals?
Hypothesis
Researchers hypothesised generally that an association between diet/lifestyle factors and disease rates would indeed exist. A specific hypothesis was that animal product consumption would be associated with an increase in cancer and chronic, degenerative disease.
Hypothesis Testing
6,500 adults in 65 different counties across China were surveyed in the 1983-4 project. These counties represented the range of disease rates countrywide for seven different cancers. The survey process with each participant included:
three-day direct observation
comprehensive diet and lifestyle questionnaires
blood and urine samples
food samples from local markets analysed for nutritional composition
survey of geographic factors
1989-1990 Survey
same counties and individuals resurveyed plus a survey of 20 additional new counties in mainland China and Taiwan.
10,200 adults surveyed
socioeconomic information collected
data combined with new mortality data for 1986-88
Analysis of Data from both 1983-1984 & 1989-1990 Surveys
data was analysed at approximately two dozen laboratories around the world to reduce chances of error in data analysis
researchers could be confident that if results were consistent, then they would be correct
Conclusion
diseases more common in Western countries clustered together geographically in richer areas of China
diseases in richer areas of the world were thus likely to be attributed to similar “nutritional extravagance”
diseases in poorer areas of the world were likely to be attributed to nutritional inadequacy/poor sanitation
blood cholesterol (strongly associated with chronic, degenerative diseases) was higher in those consuming more animal foods
lower oestrogen levels in women (associated with fewer breast cancers) related to increased plant food consumption
higher intake of fibre (found only in plants) associated with lower incidence of colon and rectal cancer
The consistency of the results led the researchers to make the overall conclusion that the closer people came to an all plant-based diet, the lower their risk of chronic disease.
Published Data
The data on both the 1983-1984 survey and the 1989-1990 survey can be seen in more detail here.
More detail on the experimental study design of the China Project (covered in Appendix B) plus a full copy of The China Study in pdf format is available here.
Professor T Colin Campbell’s complete CV (including published papers analysing data from the China Project) is available here.
Plant Protein vs Animal Protein Webinar from Professor T Colin Campbell
If you have any comments or require further information on this topic, please let me know.
Bibliography:
Chen J, Campbell TC, Li J, Peto R. Diet, Life-Style and Mortality in China: A Study of the Characteristics of 65 Chinese Counties. Oxford, UK: Oxford University Press; 1990.
Chen J, Peto R, Pan W-H, Liu B-Q, Campbell TC, Boreham J, Parpia B. Mortality, Biochemistry, Diet and Lifestyle in Rural China: Geographic Study of the Characteristics of 69 Counties in Mainland China and 16 Areas in Taiwan. Oxford, UK; Ithaca, NY; Beijing, PRC: Oxford University Press, Cornell University Press; People’s Medical Publishing House, 1990.
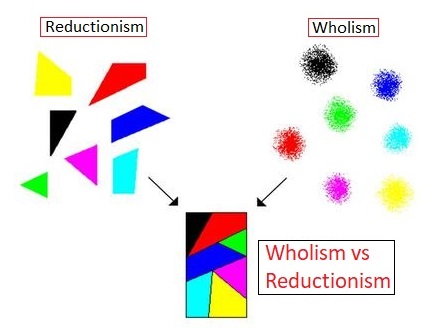
You may never have heard of these two terms, “wholism” and “reductionism”, but the war between them is not just a war of words, it’s a war of paradigms. One of these paradigms is unfortunately winning most of the battles, and the result is an escalating public health crisis.
First, let’s look at what I mean by “paradigm”. A good example is the difference between geocentric and heliocentric world views that came to a head around the 15th-16th centuries. Before the so-called Copernican Revolution (involving intellectual giants such as Nicolaus Copernicus (1473-1543), Johannes Kepler (1571-1630) and Galileo Galilei (1564-1642), the accepted and, for the most part, unchallenged paradigm was that the Sun and other planets revolved around the Earth, and the stars were all fixed in the heavens, just like it said in the Bible. Post-Revoltion, there was a slow but ultimately complete “paradigm shift” which meant that everyone now accepts that the Earth and other planets revolve around the Sun, and the stars are no longer just pin-pricks in some form of heavenly firmament.
Put simply, in terms of nutrition, wholism (a term adopted by Professor T Colin Campbell from the similar and better-known term “holism”) deals with whole diet and its effects on the whole person; whereas reductionism looks at specific elements of diet and their effect on specific parts of the person (like a specific gene for loving or hating Marmite).
The seemingly unstoppable increase in diet-related chronic diseases, such as type 2 diabetes and obesity, is simply not being addressed by the ever more precise research being undertaken by scientists, whether they are chemists looking at a specific chemical that can target particular cellular behaviour or a geneticist looking at which gene is responsible for the onset of a particular disease.
Of course it’s necessary to narrow one’s visual field to a specific area of investigation when it is appropriate (for instance, using a microscope to distinguish which virus has infected a given tissue sample); but there is a general tendency nowadays within nutritional science to exclusively apply the microscope (metaphorically speaking) to every public health issue.
Let’s look at an example: A recent report revealed that half of our schoolchildren are now dangerously overweight or obese.
A reductionist response could be to look for and try and isolate the gene that causes obesity in children. £millions or even £billions could be poured into expensive genetic research to find this “needle in the haystack”. Whereas a wholistic response could be to look at what societal changes have occurred that might account for this unwelcome change in the health of schoolchildren. You don’t have to be a rocket scientist to see that there has been a significant change in the average diets that schoolchildren are now eating when compared to previous generations.
With the reductionist response, one could expect that years and even decades could pass without anything being discovered, and all the while more and more children are likely to become obese.
With the wholistic approach, a solution could theoretically be found very quickly – legislate to improve school meals, increase junk food taxes, ban advertising of unhealthy foods to children, and so forth. The chances are that obesity statistics would start to improve the more practical efforts were made to change laws, educate parents and improve children’s diets. And whilst it might appear that governments do make some moves in this direction, their efforts to implement substantial solutions end up being quasi-wholistic because they are generally hamstrung by the pressure imposed on them by Big Pharma, Big Medicine and Big Agriculture – and the majority of research funding, whether directly or indirectly (e.g. through universities and other institutions), greatly influences which research is most powerfully supported in government circles and reflected in the media to the public.
But even if simple dietary changes could significantly reduce childhood obesity, it would probably not make the reductionists happy. They would still want to delve down into minutiae and find a biological mechanism that could then be controlled somehow, most likely by a drug that could be patented and sold for profit. There is no profit to be made from people simply changing their diets. And there is certainly no profit to be made by pharmaceutical companies or medical organisations from a population full of healthy people.
But let’s say that the geneticists do find a gene that is strongly associated with childhood obesity. It may still take years or decades of research to transfer that information into a fully-tested and certified treatment, probably in the form of a drug. And even if the obesity pill works in the trials they’ve undertaken, there is no guarantee that it will work within the general population, or that it will be free of serious side-effects only apparent years or decades later (remember Thalidomide?), or if it is too expensive for the majority of people to afford or indeed if the percentage improvement attributable to the drug would bear any comparison with the size of improvement made simply by changing dietary intake.
There is nothing wrong with geneticists exploring the fascinating world of genes, nor is there anything wrong with scientists trying to find what makes one person’s personality different from another’s, or any of the other intriguing questions that beg to be researched and answered by the curious and searching human mind.
What IS a problem, though, is when the ONLY approach to solving scientific problems, particularly those directly linked to public health, is an approach which ignores anything that is “fuzzy” and too…well, human! The funding for most of the scientific research that is undertaken nowadays is only available if there is a tangible and clear hope of achieving a binary, black and white result:
1. A always precedes B.
2. B always follows A.
3. There is no C that could also cause B.
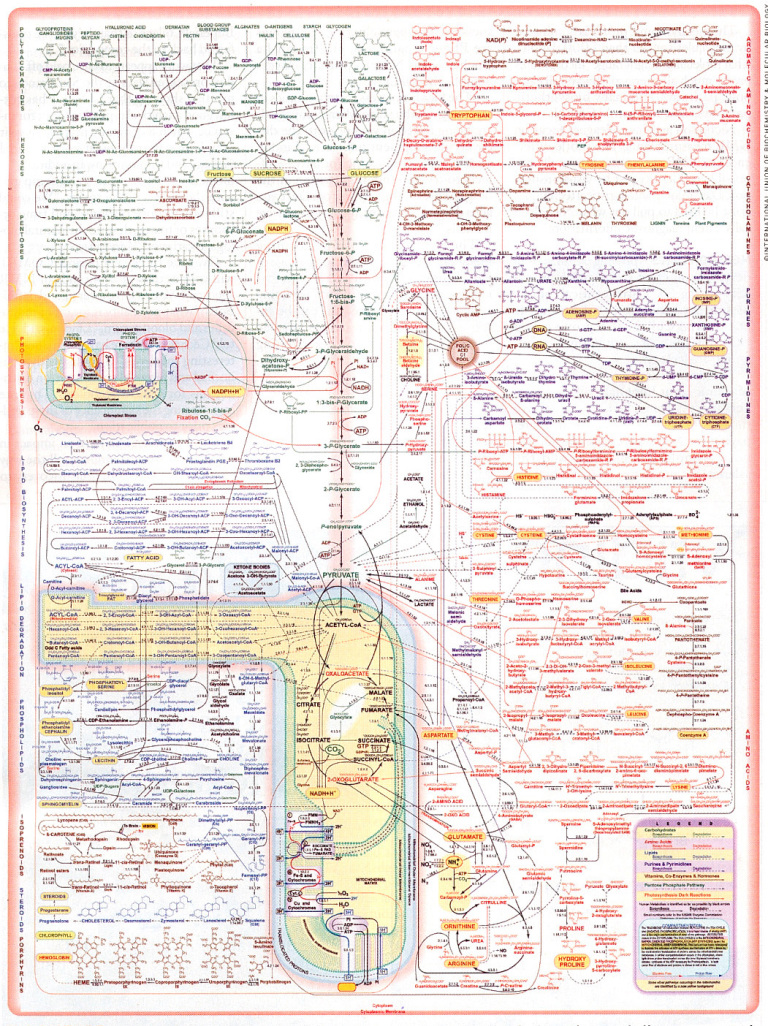
Human behaviour and particularly human nutrition on a population-wide level can never conform to this linear causal pattern. Indeed, even one single cell does not and arguably never can be analysed or understood fully by any amount of analysis – just as can be seen in quantum physics (where electrons can exist in two places at the same time – or cease to exist and reappear elsewhere in ways that can never conform to what we think of as causality), the more we delve into our biochemistry, the more we appreciate how much there is that we can never fully know. Just look at the following diagrammatic representation of just the partial metabolic processes involved in one single cell:
Professor T Colin Campbell explains (1.) the dilemma like this:
“The fact that each nutrient passes through such a maze of reaction pathways suggests that each nutrient also is likely to participate in multiple health and disease outcomes. The one nutrient/one disease relationship implied by reductionism, although widely popular, is simply incorrect. Every nutrient-like chemical that enters this complex system of reactions creates a rippling effect that may extend far into the pool of metabolism. And with every bite of food we eat, there are tens and probably hundreds of thousands of food chemicals entering this metabolism pool more or less simultaneously.”
Whilst it is understandable that the human mind is inquisitive and naturally wants to simplify complexity, is it really essential to map the inter-, intra- and extra-cellular labyrinthine world of the 100 trillion cells comprising the human body before we can identify and apply timely solutions to public health issues?
In any event, our cellular make-up is only one aspect of what constitutes the indefinably complex entity that is a human being. Can we truly ever expect to see a cellular or genetic “cog” that explains what it is to be a friend, a lover, a parent? Why we find beauty in a sunset?
Tackling childhood obesity head-on in the messy “real” world of human populations represents the sort of indeterminate complexity that does not attract large government or institutional funding. More effort goes into producing incomprehensibly complex charts such as the one above than goes into practical measures to help children live full and productive lives. This is not to say that scientists, governments and organisations do not care about the lives of real people – particularly real schoolchildren. Rather, my contention is that they are so wrapped up in doing things the way that things have been done for so long (“stuck inside the paradigm”) that they may, in part, genuinely believe that their way is the ONLY way to solve such public health crises.
This is why I believe it is appropriate to apply the term “paradigm” to the general outlook and approach that science and medicine has been immersed in for at least the past 50 years – probably since the joint effects of two discoveries: the so-called completed list of vitamins and the structure of DNA. It is also the reason why incredibly convincing population studies, such as The China Study, come under attack from reductionist thinkers. They attack such wide-scale population studies because there is no single causal link demonstrated. This is even the case when the study identifies significant differences in health markers (e.g. cancer, heart disease and type 2 diabetes) between those Chinese populations eating the traditional plant-based diets and those Chinese populations that have adopted the Standard American Diet (SAD).
There is good reason for this lack of indisputable causality: and the reason is that it is simply impossible to prove a single causal link between health and diet when, as Professor Campbell indicated above, no single nutritional input ever causes just one single biochemical response. But such linear responses are just what scientists have habitually expected to discover when the overriding world-view they have been exposed to all their academic and professional lives aims to reduce all complexity down to minute and simple mechanics.
You will have heard the saying “The whole is greater than the sum of its parts”. Intuitively obvious, but possibly not so in the majority of research laboratories around the world.
The assumption that it should be possible to find such a causal link is based on a mechanistic reductionist ideal of the Universe. The likes of Ray Kurtzweil et al consider that one day we will be able to understand everything about ourselves – biology, emotions, personality – by drilling down deeper and deeper, smaller and smaller into the world of micro and nano particles until we find all the little “cogs” and see how they are all connected. We will then be able to predict all events in the “macro world” and reproduce them in better ways with far more durable materials than human flesh and blood.
Of course we don’t want to return to an age of religion and mysticism, where all events were caused by unknown and unknowable forces, spirits and demons. Where everything in biology and personality could be accounted for by the four humours – blood, yellow bile, black bile, and phlegm! We all enjoy huge benefits from the application of reductionist approaches to finding causes and cures for TB and smallpox, and without this approach doctors might still be delivering babies with unwashed hands after having chopped up cadavers or been to the toilet, or both.
Also, I can see how a reductionist approach can be very attractive. It’s neat and orderly and avoids that great enemy of the reductionist thinker, namely, uncertainty.
But I propose that the answer to childhood obesity is both complex and simple.
It’s simple because all it requires is that we feed our children the natural diet for our species (ideally consisting completely or in the main part of whole plant foods), while ensuring that they get some regular exercise.
It’s complex because WE – our biochemistry, our personalities, our societies – ARE complex.
But effective and timely solutions to childhood obesity and many other public health crises are much more likely to be found with the help of two eyes rather than the help of a two million pound electron microscope.
Ample evidence already points to dietary change being the major factor needed in order to solve this escalating health problem. So much evidence, indeed, that I have not even bothered to list it in this article. Just scan through the databases of the NCBI or NIHR to see that sufficient research already links obesity to diet. But in spite of this, the main thrust of government and medical policy derives from what is called “Gold Standard” research, where the majority of research funding (and resultant credibility) is assigned to randomised controlled trials (RCT’s) that control all potential extraneous biases. And, clearly, you cannot do with when dealing with the nutritional and behavioural diversity that exists in the wider world of society as a whole.
This situation can be further explained by the analogy of an elephant in a room along with 60,000 blind scientists who are each responsible for describing one individual facet in minute detail. They can talk at length about the life-cycle of one of the thousands of species of bacteria colonising a crack between two toes, or churn out publications on the chemical components of a particular pigment within a hair from its tail. Yes, it’s true that they become incredibly expert in their own field of research, but it takes just one non-visually impaired child running into the room to be able to announce that there’s a bleedin’ great elephant standing there!
And to the surprise of the child, these 60,000 blind researchers with one voice ask “what’s an elephant?”
To those who have their eyes open to the whole picture, they can see that our example of childhood obesity is but one of the many chronic health conditions clearly caused by diet, and it’s always the same diet, the one that contains far too much animal protein, saturated fats, salt, sugar and processed junk, and far too little whole plant foods.
Diet is a “zero-sum” affair. Whenever one unhealthy food item goes into your mouth it means that another more healthy food item didn’t. And it is the cumulative effect of this, meal after meal, day after day, year after year that leads inexorably to the near-epidemic diet-related health issues that are starting to bring our hospitals to a standstill.
A fish is hooked, thrown onto land, flops around for a bit in the air and then escapes back into the water. Eager to tell his fishy buddies about his experience, he starts talking to them about his time out of the water. “What’s water?” they all ask, looking at him as though he’s out of his scaly mind. When water is all that you know, there is no word for it…
You may enjoy another view of this issue by Dr. Michael Greger…
Bibliography
Campbell, T. Colin. Whole: Rethinking the Science of Nutrition (p. 97). BenBella Books, Inc.. Kindle Edition.
1) What is the health claim being promoted with the supplement?
They state in a bullet-point list at the start of the advertisement the following: “A powerful source of antioxidant protection for the whole body” and “Delivers a healthy dose of essential vitamin A nutrition”. Neither of these claims is directly linked to the product since they are simply general statements and there is no definition or clarification of terms such as “healthy dose” or “essential”. It would be reasonable to assume that readers of this advertisement might consider that the seller was making these health claims about the softgel product itself.
The third bullet-pointed statement “Each convenient softgel provides 10000 IU of antioxidant nourishment” clearly links the softgel product with the claim; however, there is no immediate clarity about what “antioxidant nourishment” actually means, nor is there any supporting explanation or data related to the claim.
In the Product Description, further down the page, the seller makes additional statements:
“Get vitamin A for healthy vision and antioxidant protection for your whole body with beta- carotene!” and
“A natural plant pigment that can be converted into vitamin A by the body as needed, beta-carotene also acts as a powerful antioxidant in its own right.”
Again there is a lack of clarity about whether the above statements directly relate to the benefits of the softgel product being sold.
The exclamatory general statement in A. could be interpreted in one of two ways: firstly, that their softgel product offers these benefits or, secondly, that beta-carotene in general offers these benefits.
The general statement in B. could also be interpreted in one of the above two ways.
The lack of clarity in both the initial bullet-pointed list and in A. and B. above raise the issue of whether or not legal responsibility is being accepted for implied claims regarding the benefits of the softgel product being sold.
2) Is the health claim (as stated above) “evidence-based” (that is, based on research results)?
No. Such words as “Sources”, “References” or “Evidence” do not appear.
– Does it include any research references / citations?
No citations are used.
– Are the citations from a reputable source?
N/A
3) Who is funding the research?
There are no references to research data. A look at the seller’s website revealed no additional research-based evidence for the implied/stated claims on advertisement. And the following general statement made under the Our Guarantee tab provides no additional links to research data: “We know how important your health is to you and your loved ones. That’s why we’re focused on delivering only high quality products you can trust at the best value. Our lab evaluates every product to make sure it’s compliant with strict standards and government regulations, and we fully believe in and stand behind our products. If you’re dissatisfied for any reason, we’ll give you a full refund and pay return shipping.”
4) Who are the researchers and/or authors?
There are no researchers or authors mentioned.
– What are their credentials or qualifications?
N/A in view of the lack of information on researchers.
– Are they currently or have they previously been funded by industry?
They are a company that advertises, sells and distributes supplements to the general public. I assume they are self-funded by their own business profits. There is no indication from my research that they are in receipt of additional funding from any other source.
5) Are the conclusions well reasoned and warranted by the evidence (for the health claim listed in question #1)? Consider the following:
– Claims that sound too good to be true.
The statements they make are rather general and, on the face of it, do not seem “too good to be true”. However, because of the lack of referenced research or evidence of any sort within the advertisement there is no way of assessing the validity of their implied/stated claims for the softgel product without reference to external sources. Their general statements about the benefits of beta-carotene for healthy vision and as an antioxidant for the whole body, and for vitamin A as being in some sense “essential”, seem reasonable on the face of it. There is no mention of research suggesting the harmful effects of beta-carotene (such as can be found here and here), nor of the biochemical relationship between beta-carotene as a precursor for vitamin A except for the generalised statement that beta-carotene is a “…natural plant pigment that can be converted into vitamin A by the body as needed”. The term “natural” when applied to a vitamin supplement containing isolated beta-carotene is something that is not justified and might mislead the reader to suspect that supplementation is as natural a way of acquiring beta-carotene as deriving it from diet.
– Recommendations that promise a quick fix.
“Delivers a healthy dose of essential vitamin A nutrition” and “Each convenient softgel provides 10000IU of antioxidant nourishment” appears to be offering a solution to a problem – viz. the problem of not having sufficient vitamin A nutrition and/or sufficient antioxidant nourishment. I think it would be reasonable to suspect that the average reader would consider this to be a quick fix for a perceived deficiency in vitamin A nutrition and/or sufficient antioxidant nourishment – whatever these terms do or do not imply or actually mean when put under scrutiny.
6) What might be some important consequences of accepting these conclusions (for individuals, society, the environment, etc.)?
In terms of consequences for individuals purchasing and taking this supplement, there are potentially significant implications. Whenever unsupported health claims are made in relation to health supplements, there is a danger of individuals being misled. When a supplement is fairly innocuous and has no associated published evidence included with it to suggest inherent dangers associated with its use, issues of reliability of claims and value for money are perhaps the most relevant issues involved. However, when the supplement being sold has been shown in published literature to have associated dangers, this is something that might raise much greater concern. In this case, I believe that there is ample research data on the negative effects of vitamin A / beta-carotene supplements to raise the question of whether or not the seller should be legally allowed to advertise this product without some printed warning being included in the advert.
As Professor T Colin Campbell asks“Did you know, for example, that vitamin A at higher levels of intake, actually can increase, not decrease, cancer risk?”
In terms of environmental consequences, I can see none.
In terms of societal consequences, there is the wider issue of how much responsibility should be taken by governments and organisations (such as Amazon – the website advertising this product) for allowing companies like Swanson vitamins to sell products without any health warnings or reference to evidence in support of implied or stated health claims for the product in question.
Final Comment
So, I hope you found this example of critical thinking of some interest. I would suggest that it is a good idea to apply similar analytical approaches to anything you come across, written or verbal, that makes claims about your health.
You only have one life, and I hope you do all you can to live it to the fullest, healthiest and happiest…seeing through the empty promises of organisations and individuals who would sell you anything just to make a quite profit.
This is one the healthiest bread recipes I have come up with. It may not have the oily and salty attraction of some other breads – because, well… it has NO OIL OR SALT!
We can all get rather addicted to the convenience, texture and taste of commercially-prepared breads. The tastier and more “spongy” they make the bread, the more they will sell.
But I wanted a bread that provides most of the convenience, texture and taste that we expect from bread, but without the fragmented food elements and chemicals that may be added, including: salt (1.), sugar, (my recipe contains a small amount but commercial bread can contain lots), trans fats (“partially hydrogenated oils” – linked to serious health risks (2., 3.)), potassium bromate (oxidising agent), azodicarbonamide (dough conditioner/bleacher), monoglycerides & diglycerides (emulsifiers E471), butylated hydrocyanisole (BHA preservative linked to cancer (4., 5.)), caramel colouring (linked to cancer (6., 7.)), high fructose corn syrup (HFCS linked to heart disease and diabetes (8.)), Undeclared GMO Soy oil (9.), vegetable oils (10,. 11,. 12,). And this is not a definitive list..
And if you still think that adding vegetable oils (even really expensive extra virgin olive oil) is a healthy option, you may want to check out some of my future blogs. In the meantime, a brief word from Dr Caldwell Esselstyn.
So, after all that waffle, here’s the recipe:
Whole Wheat Seeded Health Bread.
This basic recipe forms the canvas on which the rest of the health bread recipes I use are formed. This recipe is incredibly versatile, and makes a delicious, moist health bread that can be enjoyed with any kind of meal. It is also delicious served with natural fruit preserves and organic, natural nut butters. These health breads don’t require kneading, as the ingredients form more of a batter than a dough once mixed together.
Preheat the oven to 390 degrees (200 degrees Celsius gas mark 6). This recipe yields three loaves, so you will need three silicon medium-sized loaf tins – silicon so that they do not stick, being that no grease or oils are used.
Ingredients:
4 cups (1kg) organic wholewheat flour. I vary this from time to time by adding differing amounts of wholemeal ancient flours – usually rye and spelt, but also sometimes Khorasan also called kamut (adds sweetness) or einkorn.
35-75ml organic raw brown sugar (I use as little as possible and let it rise for longer).
Dissolve the sugar in the lukewarm water and sprinkle the yeast over the top. Cover tightly with cling film and a dish towel, and set aside for the yeast to activate, it will start to bubble when it has activated.
In a large mixing bowl, mix together the flour and seeds. Add the water, sugar and yeast mixture and mix very well to form a slightly runny batter. Divide the batter equally amongst the loaf tins which should be on a firm metal baking tray. Place the bread tins somewhere warm and draught-free until the batter has risen and the loaves have doubled in size. Bake for 45-50 minutes, until a dark crust has formed and the bread sounds hollow when tapped. You can also check that they are completely baked by using a skewer or knife. If there is any batter sticking to the latter, put them back in the oven for another 10 mins or so. Allow the loaves to cool in the tins for ten minutes before turning out onto a cooling rack.
Try it. Vary it. Improve on it. And let me know how you get on.
The following is Yuri’s “Flower Bread” – basically the same recipe with added red pepper and garlic, but made in a wonderful flower-shaped silicone bread/cake tin that he found in Italy.
Fantastico!
References
https://nutritionfacts.org/topics/salt/ “Dozens of similar studies demonstrate that if you reduce your salt intake, you may reduce your blood pressure. And the greater the reduction, the greater the benefit may be. But if you don’t cut down, chronic high salt intake can lead to a gradual increase in blood pressure throughout life.”
Vandana Dhaka, Neelam Gulia, Kulveer Singh Ahlawat, and Bhupender Singh Khatkarcorresponding. J Food Sci Technol. 2011 Oct; 48(5): 534–541. Published online 2011 Jan 28. doi: 10.1007/s13197-010-0225-8. Trans fats—sources, health risks and alternative approach – A review
Trattner S, Becker W, Wretling S, Öhrvik V, Mattisson I. Food Chem. 2015 May 15;175:423-30. doi: 10.1016/j.foodchem.2014.11.145. Epub 2014 Dec 3. Fatty acid composition of Swedish bakery products, with emphasis on trans-fatty acids.
Otterweck AA, Verhagen H, Goldbohm RA, Kleinjans J, van den Brandt PA. Food Chem Toxicol. 2000 Jul;38(7):599-605. Intake of butylated hydroxyanisole and butylated hydroxytoluene and stomach cancer risk: results from analyses in the Netherlands Cohort Study.
Garima Sengarcorresponding author and Harish Kumar Sharma. J Food Sci Technol. 2014 Sep; 51(9): 1686–1696. Published online 2012 Feb 9. doi: 10.1007/s13197-012-0633-z. Food caramels: a review.
James M. Rippe Theodore J. Angelopoulos. Advances in Nutrition, Volume 4, Issue 2, 1 March 2013, Pages 236–245, https://doi.org/10.3945/an.112.002824. Sucrose, High-Fructose Corn Syrup, and Fructose, Their Metabolism and Potential Health Effects: What Do We Really Know? N.B. The symposium was supported in part by an educational grant from the Corn Refiners Association (I ALWAYS SUSPECT BIAS WHEN THUS FUNDED).
https://nutritionfacts.org/video/gmo-soy-and-breast-cancer/. “The bottomline is that there is no direct human data suggesting harm from eating GMOs, though in fairness such studies haven’t been done, which is exactly the point, critics counter. That’s why we need mandatory labeling on GMO products so that public health researchers can track whether GMOs are having any adverse effects.”
https://nutritionfacts.org/topics/vegetable-oil/. “Research confirms that ingestion of oil, no matter which type of oil or whether it was fresh or deep fried, showed a significant and constant decrease in arterial function.”


 First, let me introduce you to someone I expect many of you have never even heard of – Dr Rui Hau Liu, PhD, MD (see bottom of post for more information about his academic and professional qualifications).
First, let me introduce you to someone I expect many of you have never even heard of – Dr Rui Hau Liu, PhD, MD (see bottom of post for more information about his academic and professional qualifications).
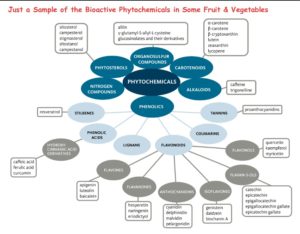 We have little idea yet about how the 8,000 or so known bioactive compounds in fruits, vegetables and whole grains relate to and depend upon each other. And, again, it is thought that there are many thousands more yet to be discovered. It is not, therefore, difficult to understand that food components and nutrients work synergistically in whole foods, through a complex variety of different mechanisms. We cannot replicate the benefits of food with isolated chemical supplements.
We have little idea yet about how the 8,000 or so known bioactive compounds in fruits, vegetables and whole grains relate to and depend upon each other. And, again, it is thought that there are many thousands more yet to be discovered. It is not, therefore, difficult to understand that food components and nutrients work synergistically in whole foods, through a complex variety of different mechanisms. We cannot replicate the benefits of food with isolated chemical supplements.